
Abstract

A 38-year-old with a history of intravenous drug use and HIV presented to our institution with a 3-week history of worsening headache and a progressively enlarging mass on the right side of his head. The patient noted that the mass had started to press on his right eye and had become red and painful to touch. The patient denied any fevers, nausea, vomiting, neck pain, or neurological symptoms. Review of systems also revealed a 20-pound weight loss over the previous 6 months, as well as 2-week history of oral ulcers. On physical examination, a large erythematous mass of the frontotemporal scalp was noted extending over the right eyelid. A thick white plaque was identified on the surface of the tongue in addition to multiple oral ulcers. The patient also appeared cachectic. No neurological deficits were noted.
The patient’s vital signs were within normal limits on presentation and no leukocytosis was present on laboratory workup. The patient’s CD4 count was 86. A computed tomography (CT) study of the head without contrast was obtained and showed extensive soft tissue swelling involving the right frontotemporal scalp extending into the temporalis muscle and masticator space in addition to a 1.7 cm × 0.4 cm epidural collection subjacent to the scalp swelling. No bony changes were evident on CT. A magnetic resonance imaging (MRI) study of the brain with and without contrast was then obtained, which demonstrated similar findings of an inflammatory process involving the temporal fossa and epidural space, however with intervening bone marrow involvement now evident (Figure 1).
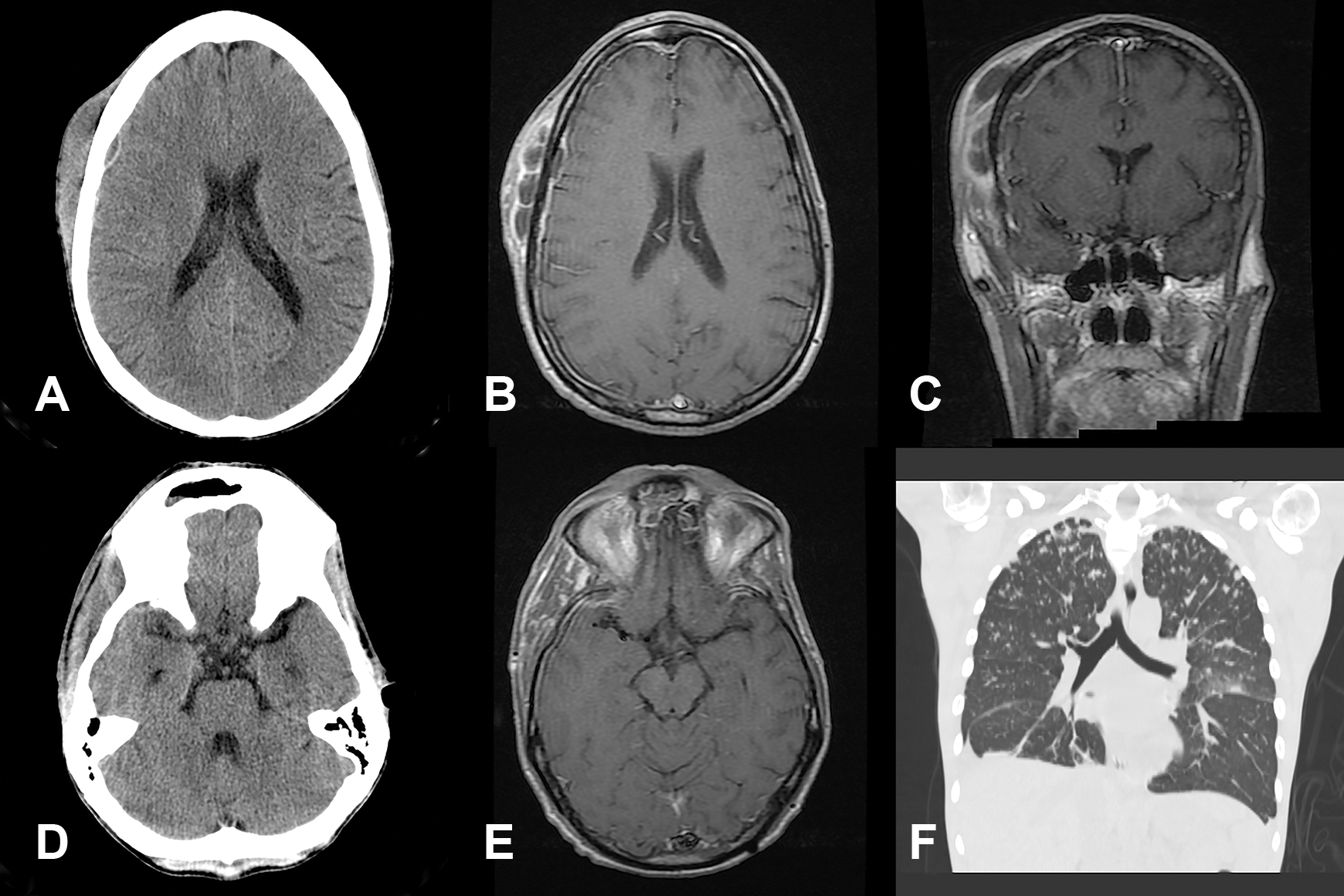
A, Axial noncontrast CT scan of the head at the level of the lateral ventricles demonstrates extensive frontotemporal extracranial swelling and a subjacent 1.7 cm × 0.4 cm epidural fluid collection with hyperattenuating rim. No bony abnormalities were noted in this region on bone windowing. B, Corresponding postcontrast MRI in the axial plane demonstrates a multiloculated, peripherally enhancing fluid collection involving the subcutaneous and cutaneous soft tissues, subgaleal space, and temporalis muscle with contiguous osseous spread into the epidural space. A 1.7 cm × 0.4 cm peripherally enhancing epidural fluid collection is present with adjacent pachymeningeal enhancement. C, Postcontrast MRI of the brain in the coronal plane better demonstrates hypointensity and patchy enhancement of the intervening parietal bone marrow consistent with osteomyelitis. D and E, Axial noncontrast CT scan of the head and corresponding postcontrast axial magnetic resonance image at the level of the suprasellar cisterns demonstrates right temporalis muscle edema consistent with an inflammatory process involving the masticator space. F, The CT scan of the chest, coronal plane. Extensive pulmonary nodules in a “tree-in-bud” distribution are demonstrated, with primary consideration to disseminated pulmonary nocardiosis versus mycobacterial infection. CT indicates computed tomography; MRI, magnetic resonance imaging.
Surgical exploration of the lesion was conducted, which revealed a large amount of purulent material underneath the scalp infiltrating into the temporalis muscle and erosive changes of the parietal bone. Burr hole drainage was performed for the epidural abscess; exploration revealed no subdural involvement.
Pathologic examination of tissue samples from the abscess and temporalis muscle showed numerous Gram-positive filamentous bacteria, and immunostaining demonstrated numerous treponemal spirochetes. Cultures and sequencing identification confirmed the presence of numerous Nocardia organisms. A CT study of the chest showed features consistent with pulmonary nocardiosis (Figure 1F). The lungs were likely the site of this patient’s primary infection, 1 with the abscess having been seeded by hematogenous spread. 2
In addition to the uncommon coinfection of Nocardia and Treponema species in this patient’s cranial lesion, this case is notable for the significant extension of the infection through contiguous structures. This resulted in synchronous intra- and extracranial involvement that was demonstrated on imaging studies. Given the patient’s presentation with already extensive disease (involving the epidural space, cranial bone, and extracranial soft tissue and muscle), it was unclear as to which tissue the infectious process originated from. The epidural space is an uncommon location for nocardial abscess. In a recent review of 84 cases of central nervous system nocardiosis, only 2 patients were found to have epidural involvement. 3 Nocardia osteomyelitis is even rarer and is almost always caused by local invasion or direct inoculation, with only one case of hematogenous spread to the bone reported in the literature. 4 In contrast, hematogenous spread of Nocardia to the skin and soft tissues is a common and well-known manifestation of disseminated disease. 5 It is therefore likely that this patient’s lesion originated in the extracranial soft tissues, with later local invasion through the bone and intracranial structures. The authors believe that the above case provides a unique manifestation of a commonly encountered infection in the immunosuppressed patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.