
Abstract

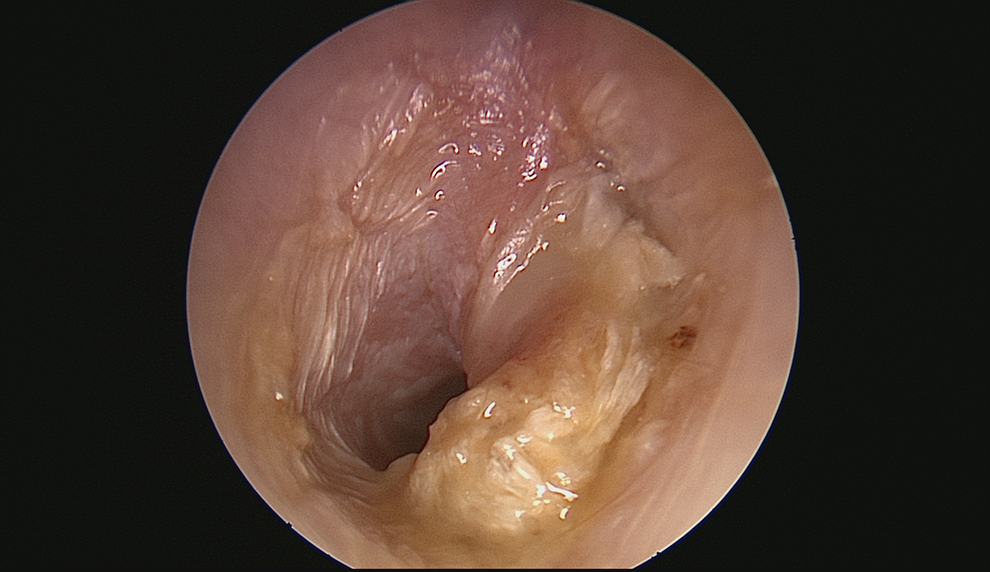
A 29-year-old woman was referred to the senior author’s practice for a right ear cholesteatoma. The patient first noticed intermittent right ear symptoms 2 years prior with persistent right ear infections, rotary vertigo, nausea/vomiting, hearing loss, and tinnitus. Examination revealed moderate conductive hearing loss with 100% discrimination in the right ear. On microscope examination, the right tympanic membrane (TM) showed a well-demarcated mouth of cholesteatoma at the pars flaccida, with an incudopexy but an otherwise clear middle ear (Figure 1). Computed tomography imaging revealed dehiscence of the right superior semicircular canals and some scutal erosion without any fistula of the lateral semicircular canal. She was lost to follow-up.

March 2017 initial presentation. Cholesteatoma with crusting over the sac.
One year later, the patient returned with exacerbation of symptoms. In the interim, she had a right lingual nerve injury during a molar extraction. She had undergone nerve repair, but immediately upon awakening from the repair procedure, she noted markedly worsened quality of right ear hearing accompanied by sharp, stabbing pains in that ear. Additional symptoms arose on a subsequent flight: during descent, she noted warm fluid emanating from her right ear along with staining of her earplug. One week after the flight, microscope examination of the right ear revealed keratin and the contents of the sac being expelled through the mouth of the cholesteatoma, out into the ear canal (Figure 2). The mechanism for expelling of the sac contents was presumed to be infection, possibly assisted by pressure changes during descent. The debris was cleared (Figure 3) and she elected to proceed with surgery.
May 2018 precleaning with the cholesteatoma’s inlet at the pars flaccida, showing exophytic, keratinaceous material protruding into the ear canal.
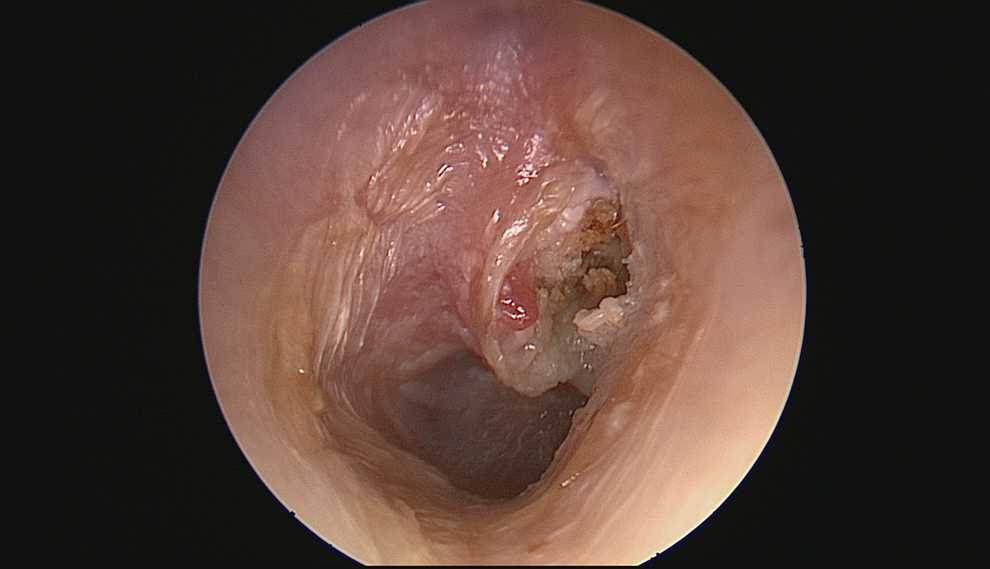
May 2018 postcleaning with partially expelled keratin and granulation tissue contents.
Operative findings included a right attic cholesteatoma emanating from a discrete retraction pocket of the pars flaccida, with a bulky sac impacted within the epitympanum, with broad areas of tegmen thinning and focal areas of dural exposure. The cholesteatoma extended into the antrum but not the mastoid. The pars tensa was intact with preserved aeration of the inferior part of the middle ear. There was significant erosion of the body of the incus as well as erosion of the posterior surface of the long process, which still held an intact connection from the lenticular process to the intact and mobile stapes. The head of the malleus also showed partial erosion.
Cholesteatomas are keratinizing, non-neoplastic lesions, characterized by the expansion of squamous epithelium into the middle ear and/or mastoid cavity. Acquired cholesteatomas result from invasion of squamous epithelium from the TM or the external auditory canal (EAC) into these spaces, leading to bone erosion. Otoscopic examination is essential for diagnosis, with the typical appearance of keratin accumulating within a retraction pocket of the pars flaccida or pars tensa, with associated scutal or ossicular erosion. 1
Recent literature on cholesteatoma pathogenesis has shifted the focus to inflammatory mechanisms. The nucleotide-binding oligomerization domain-like receptor protein 3 inflammasome, a molecular modulator of interleukin 1β, has been implicated in middle ear cholesteatoma and in chronic otitis media. 2 A 2015 study implicated Toll-like receptor 4 (TLR-4), with an increased number of TLR-4-positive cells correlated with a greater degree of cholesteatoma formation, invasion, bone destruction, and hearing loss. 3 Another recent study identified triggering receptors expressed on myeloid cells whose downregulation in mice models impaired the maturation of experimentally acquired cholesteatomas. 4
Cholesteatomas typically have a characteristic appearance with crusting within the mouth of a sac (Figure 1). However, primary acquired cholesteatomas can also have atypical appearances (Figure 2). As seen in this case, atypical presentations can take the form of exophytic, keratinous masses protruding beyond the TM into the EAC. With these atypical presentations, the diagnosis of cholesteatoma should not be overlooked.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.