
Abstract

Introduction
Submandibular swelling presents a diagnostic challenge to the pediatric population. A broad differential must be considered including infectious, inflammatory, and neoplastic processes. 1 Prompt diagnosis of infection requires a high index of suspicion and is critical to initiating steps toward definitive management. In the submandibular region, odontogenic infections are most commonly the site of origin. 2 However, sialadenitis, lymphadenitis, or trauma can also introduce infection into this area. Less commonly, foreign bodies, both penetrating and ingested, may serve as a nidus of infection. This report illustrates the importance of inquiring about foreign bodies when evaluating a child with a neck infection.
Case Report
A 9-month-old male presented with a left neck swelling and redness that had progressed over 2 days. He was eating and drinking normally with no recent infections. He had no recent travel or animal exposure. On examination, there was a 2-cm by 5-cm area of swelling and erythema at the angle of the mandible below the ear. Centrally, there was a 1-cm linear swelling that was tender to the touch (Figure 1). There were no signs of penetrating injury. Ultrasound showed soft tissue swelling but no collections. He was admitted for intravenous antibiotics. On day 2 of admission, a small central area opened and purulent material was expressed. Computed tomography scan demonstrated fat stranding with inflammation of the sternocleidomastoid and posterior belly of digastric (Figure 2). Given the examination, he was brought to the operating room. Upon opening the wound, a 5-cm white feather was extracted (Figure 3). The wound was explored, and a small amount of mucopurulent material was released and a second feather was discovered. Cultures grew Staphylococcus aureus, Streptococcus agalactiae, and Gemella morbillorum. The patient did well and was discharged home on oral antibiotics.

Appearance of a 9-month-old with an infection in the submandibular area at presentation. The arrow marks a 1-cm linear area in the center of the swelling that was raised and exquisitely tender to the touch.

Preoperative computed tomography (CT) scan of a child with an infection in the submandibular area. Although purulent material was expressed at the bedside, no obvious fluid collections were apparent. The white arrow indicates a raised area that could be felt clinically. Fat stranding can be seen in the subcutaneous tissue around the area and submandibular space. There are prominent reactive appearing lymph nodes. There is thickening of the platysma, but the remaining structures of the neck are unremarkable.
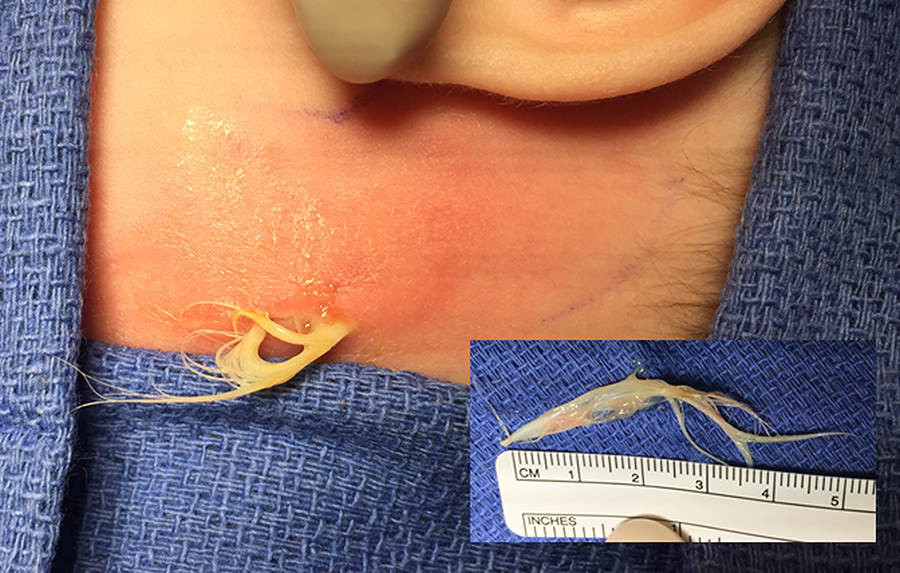
Intraoperative photographs of an embedded feather foreign body. The first feather is shown in the inset measuring approximately 5 cm in length. A second smaller feather measuring 3 cm was found upon exploration of the wound cavity (not shown).
Discussion
Since 1955, there have been 5 reports of embedded feathers resulting in infections of the head and neck and an additional case reported in the popular media. 3 –8 Five cases developed an abscess necessitating surgery and intravenous antibiotics. Recurrent abscess developed in 2 cases, 3,6 and one case developed an external carotid artery pseudoaneurysm. 3 In the majority of cases, the infections occurred near the angle of the mandible. A variety of microorganisms were cultured from these wounds and were often polymicrobial. The putative mechanism was penetrative injury owing to the sharpness of avian pin feathers and delicacy of infant skin. These sharp feathers extrude from pillows and bedding potentially penetrate the skin without leaving an external opening. Pascoe described a parotid abscess resulting from an embedded feather and suggested that the feather migrated to the parotid through Stensen’s duct. 7 Other authors have also described foreign bodies such as blades of grass and fish bones passing through the parotid and submandibular ducts. 9,10 An alternative mechanism may be that the feathers were ingested and became stuck in the oropharynx or hypopharynx and then migrated through the tissues of neck. Although sharp objects such as fish and chicken bones or barbecue brush bristles are the more obvious culprit in this type of injury, in 2006, a case of an ingested blade of grass was found to have caused recurrent neck infections and ultimately an abscess. 11 –13 This article highlights the risk of feather pillows and bedding in infants and the importance of considering an embedded foreign body as a differential diagnosis of a neck space infection particularly when no other infectious sources are evident.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.