
Abstract

Ectopic nasal teeth are extremely rare with an estimated incidence of <1%. 1 These are postulated to result from abnormal neural crest migration, defective epithelial–mesenchymal fusion, and devolution to the dentition of extinct primates. 2 Infection, malignancy, trauma, and congenital defects are also potential etiologies. 3 When bothersome symptoms occur, surgical removal is necessary.
A 30-year-old woman presented with a 1-year history of recurrent left nasal obstruction, epistaxis, and sinus infections. Physical examination revealed a large calcified object embedded in the left nasal cavity and surrounded by purulence and debris (Figure 1). Intraoral examination demonstrated an absent left lateral incisor. Biopsy showed calcified secretions and clumps of bacteria. Computed tomography demonstrated an 8 mm × 4 mm × 15 mm mass in the left nasal cavity between the inferior turbinate and nasal septum (Figure 2).
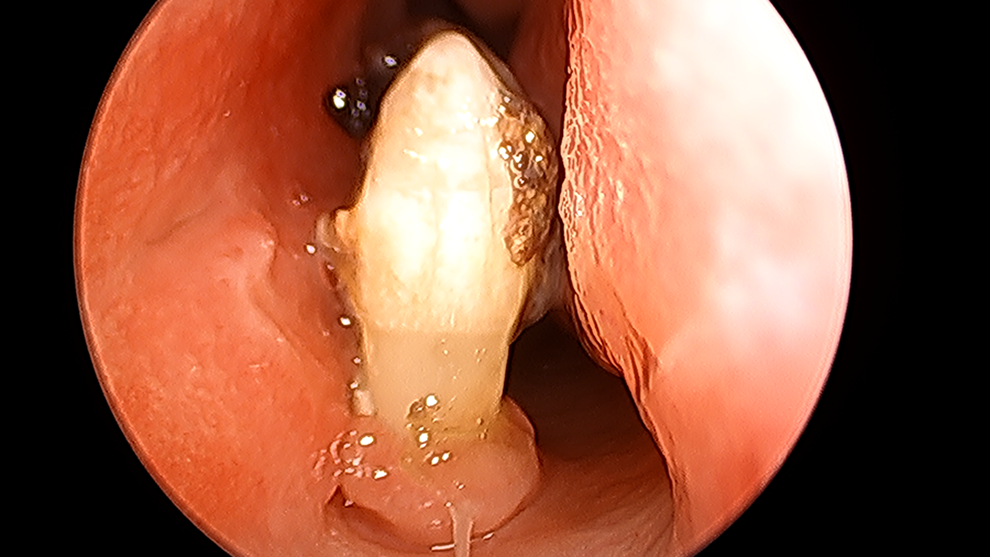
Endoscopic view of the tooth embedded in the nasal floor.
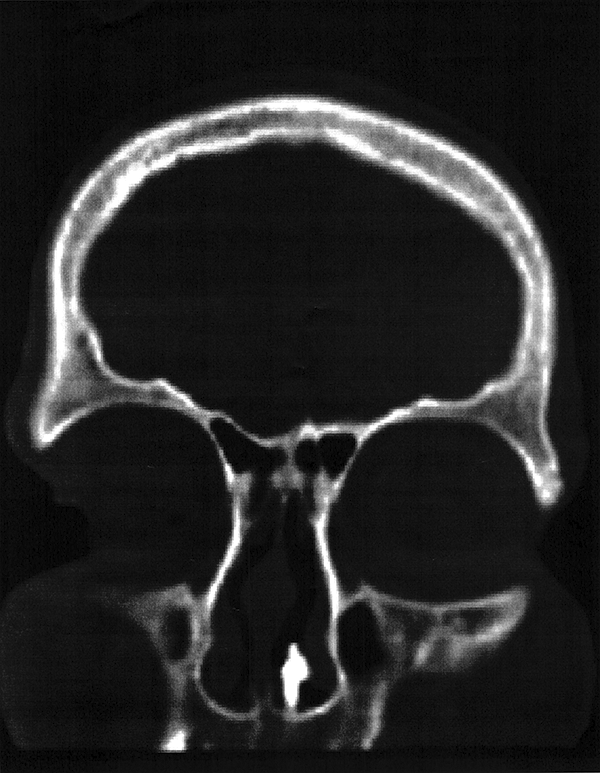
Coronal CT showing an abnormal left intranasal mass. CT indicates computed tomography.
The patient underwent endoscopic removal of the lesion. A high-speed drill was used to smooth the extraction site, and adjacent nasal mucosa was rotated to cover the exposed bony pit. The mass contained densely adherent crusts and granulation tissue (Figure 3). Final pathology was consistent with a tooth surrounded by inflammatory tissue. The patient demonstrated complete resolution of abnormal findings and has remained asymptomatic at the 1-year follow-up.

Surgically extracted specimen with densely adherent granulation tissue and debris.
A review of 13 patients with intranasal ectopic teeth found that 70% occurred in males and was far more common on the left side. Of these patients, 84% had supernumerary teeth. 4 The maxillary sinus and premaxilla were also common sites in up to 18% of cases. 3 The differential diagnosis includes foreign body, bony sequestration, neoplasm, exostosis, and rhinolith. 4 Common symptoms include unilateral obstruction, nasal drainage, crusting, pain, and epistaxis. Chronic or severe cases may result in nasal septal abscess, fistula, osteomyelitis, and septal perforation. 4,5 Transnasal endoscopic resection is well suited in most cases as it provides enhanced visualization, low morbidity, and precise dissection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.