
Abstract
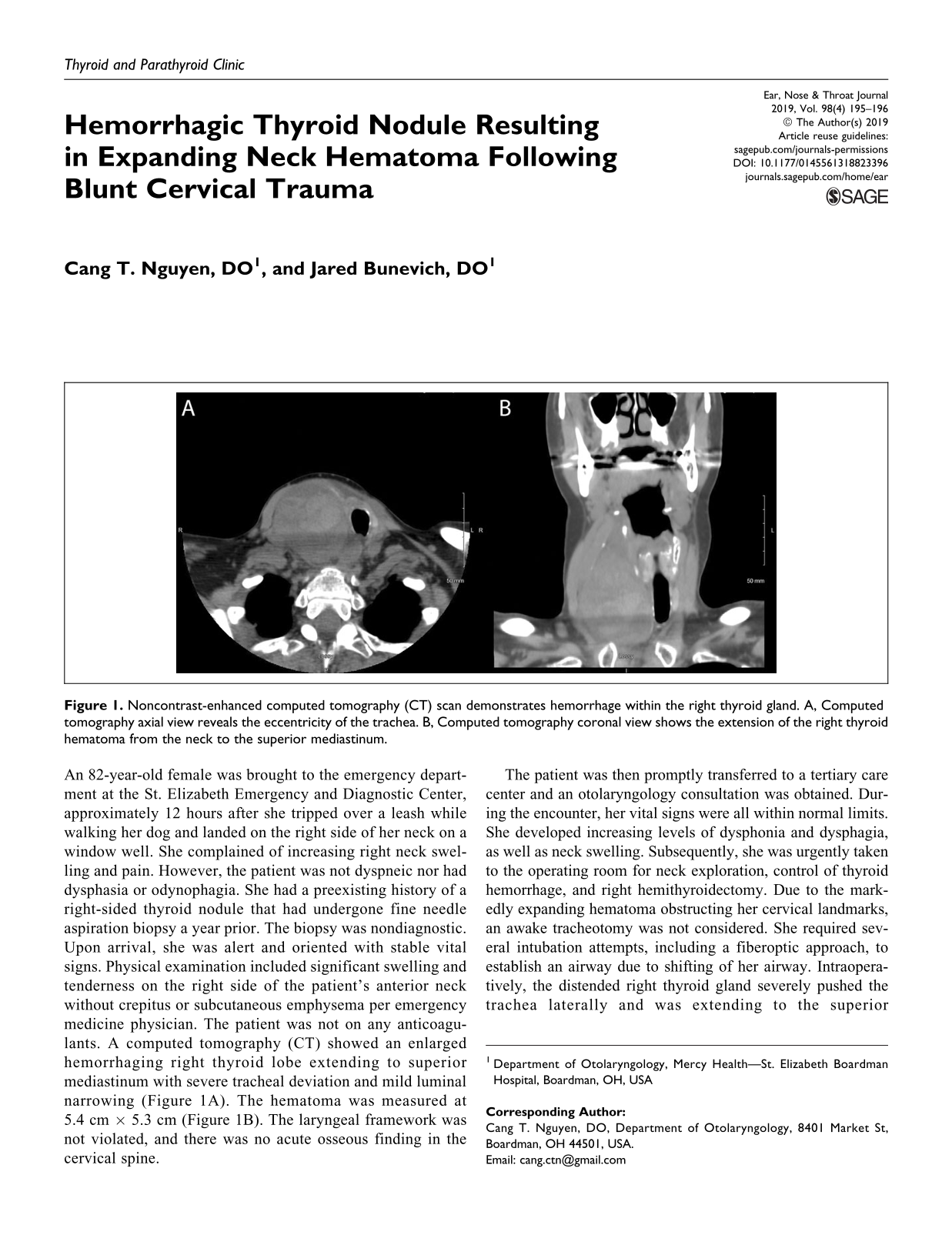
An 82-year-old female was brought to the emergency department at the St. Elizabeth Emergency and Diagnostic Center, approximately 12 hours after she tripped over a leash while walking her dog and landed on the right side of her neck on a window well. She complained of increasing right neck swelling and pain. However, the patient was not dyspneic nor had dysphasia or odynophagia. She had a preexisting history of a right-sided thyroid nodule that had undergone fine needle aspiration biopsy a year prior. The biopsy was nondiagnostic. Upon arrival, she was alert and oriented with stable vital signs. Physical examination included significant swelling and tenderness on the right side of the patient’s anterior neck without crepitus or subcutaneous emphysema per emergency medicine physician. The patient was not on any anticoagulants. A computed tomography (CT) showed an enlarged hemorrhaging right thyroid lobe extending to superior mediastinum with severe tracheal deviation and mild luminal narrowing (Figure 1A). The hematoma was measured at 5.4 cm × 5.3 cm (Figure 1B). The laryngeal framework was not violated, and there was no acute osseous finding in the cervical spine.
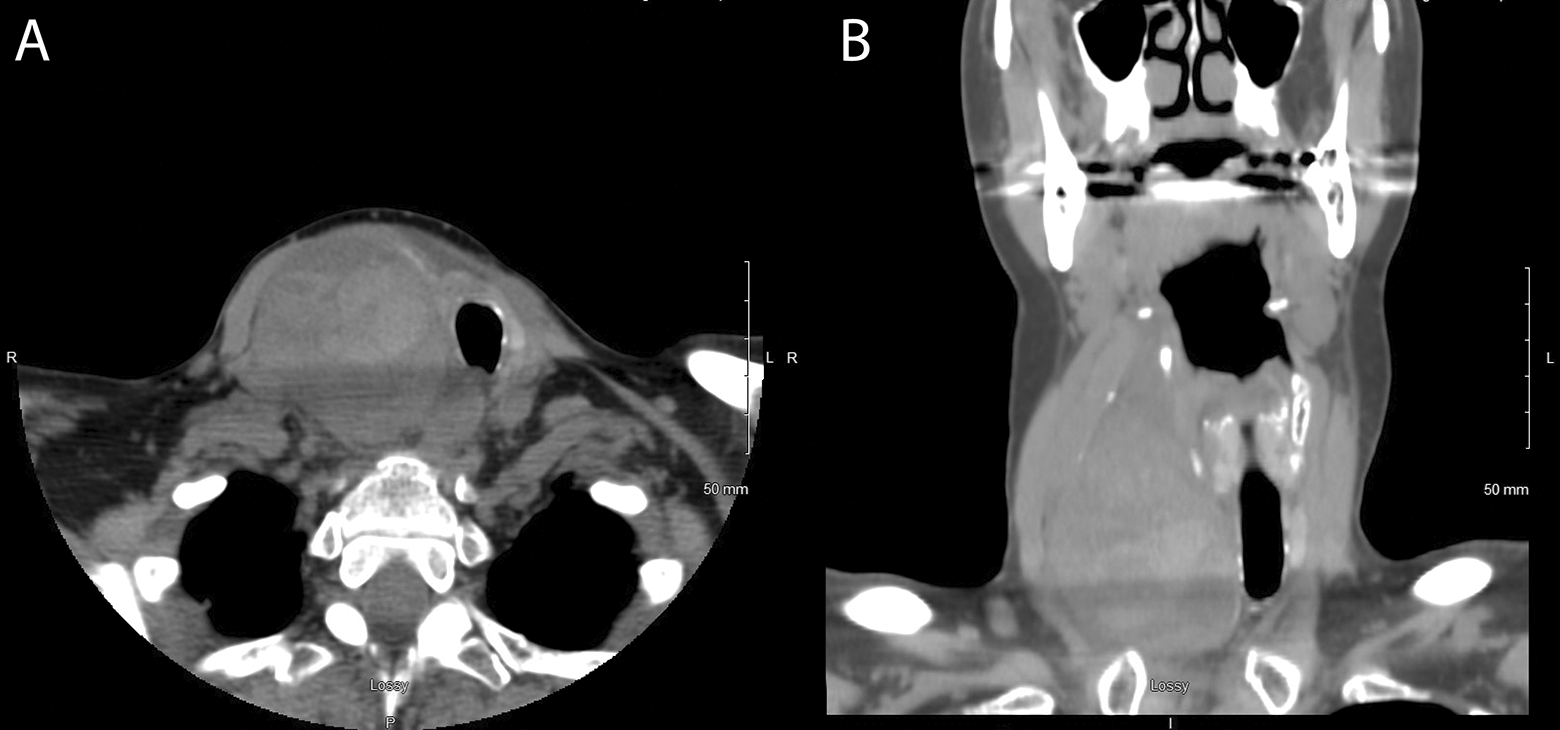
Noncontrast-enhanced computed tomography (CT) scan demonstrates hemorrhage within the right thyroid gland. A, Computed tomography axial view reveals the eccentricity of the trachea. B, Computed tomography coronal view shows the extension of the right thyroid hematoma from the neck to the superior mediastinum.
The patient was then promptly transferred to a tertiary care center and an otolaryngology consultation was obtained. During the encounter, her vital signs were all within normal limits. She developed increasing levels of dysphonia and dysphagia, as well as neck swelling. Subsequently, she was urgently taken to the operating room for neck exploration, control of thyroid hemorrhage, and right hemithyroidectomy. Due to the markedly expanding hematoma obstructing her cervical landmarks, an awake tracheotomy was not considered. She required several intubation attempts, including a fiberoptic approach, to establish an airway due to shifting of her airway. Intraoperatively, the distended right thyroid gland severely pushed the trachea laterally and was extending to the superior mediastinum (Figure 2). The nodule was inadvertently ruptured. The right inferior thyroid artery was identified, which was hemorrhaging into the nodule. The artery was then clamped, cut, and tied with 2-0 silk. The hematoma was evacuated. The right thyroid lobe was then completely excised and freed from the trachea. She was admitted overnight for observation and was discharged home the next day in stable condition. Pathology report revealed Hürthle cell adenoma with extensive hemorrhage and necrosis. The patient did remarkably well during follow-up visits.

Intraoperative view of the right thyroid hematoma that is severely pushing the trachea to the left. The course of the trachea is highlighted (dotted) from the sternal notch (arrow) to the cricoid cartilage (arrow head).
Although airway compromise is usually a late presentation, it could be fatal as the expanding hematoma compresses the tracheal airway, leading to respiratory compromise. A classification and treatment algorithm of blunt thyroid injury was proposed by Heizmann et al, which included different grades of neck injury as shown in contrast-enhanced CT, 1 and was later modified by Lemke et al. Lemke and colleagues added patients’ presenting clinical symptoms to the treatment algorithm. 2 Thyroid injury treatments range from conservative observation 3 to surgical exploration, as in this case. Due to the urgency of our patient’s rapid deterioration, we opted for immediate surgical intervention rather than reordering contrast-enhanced CT to further assess her expanding neck hematoma.
Recognizing the preceding symptoms is critically important in the management of hemorrhaging thyroid hematoma. A CT scan, preferably with contrast-enhanced, should always be performed and may be supplemented with flexible fiberoptic nasopharyngolaryngoscopy. However, surgical intervention should not be delayed if patient is presenting with increasing stridor, dyspnea, dysphonia, or neck swelling.
Footnotes
Acknowledgment
The authors would like to thank Seth Sharp, CRNA for the clinical photograph.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.