
Abstract
Introduction
Fungal rhinosinusitis (FRS) can be divided into invasive FRS (IFRS) and non-IFRS, whereas IFRS can be further classified into chronic IFRS, granulomatous IFRS, and acute (fulminant) IFRS. 1 The invasive and deadly IFRS has aroused great attention in recent years along with increased knowledge of FRS. However, chronic invasive FRS (CIFRS) is often neglected or misdiagnosed due to its insidious onset and gradual progression. In the current study, we retrospectively analyzed the clinical data of patients with CIFRS who were diagnosed in the Department of Rhinology of Beijing Tongren Hospital during the period from 2006 to 2014 and proposed feasible diagnosis and treatment strategies, with an attempt to further increase the awareness of this disease among clinicians and thus improve its management.
Participants and Methods
The clinical data of patients with CIFRS who were diagnosed in the Department of Rhinology of Beijing Tongren Hospital during the period from 2006 to 2014 were retrospectively collected. Finally, 16 patients (7 males and 9 females) were recruited. The age ranged from 21 to 71 years (mean: 55.4 ± 13.4 years). The follow-up lasted for 1 to 8 years. The demographic data, disease history, imaging findings, pathological findings, and pathogenic findings are presented in Tables 1 and 2.
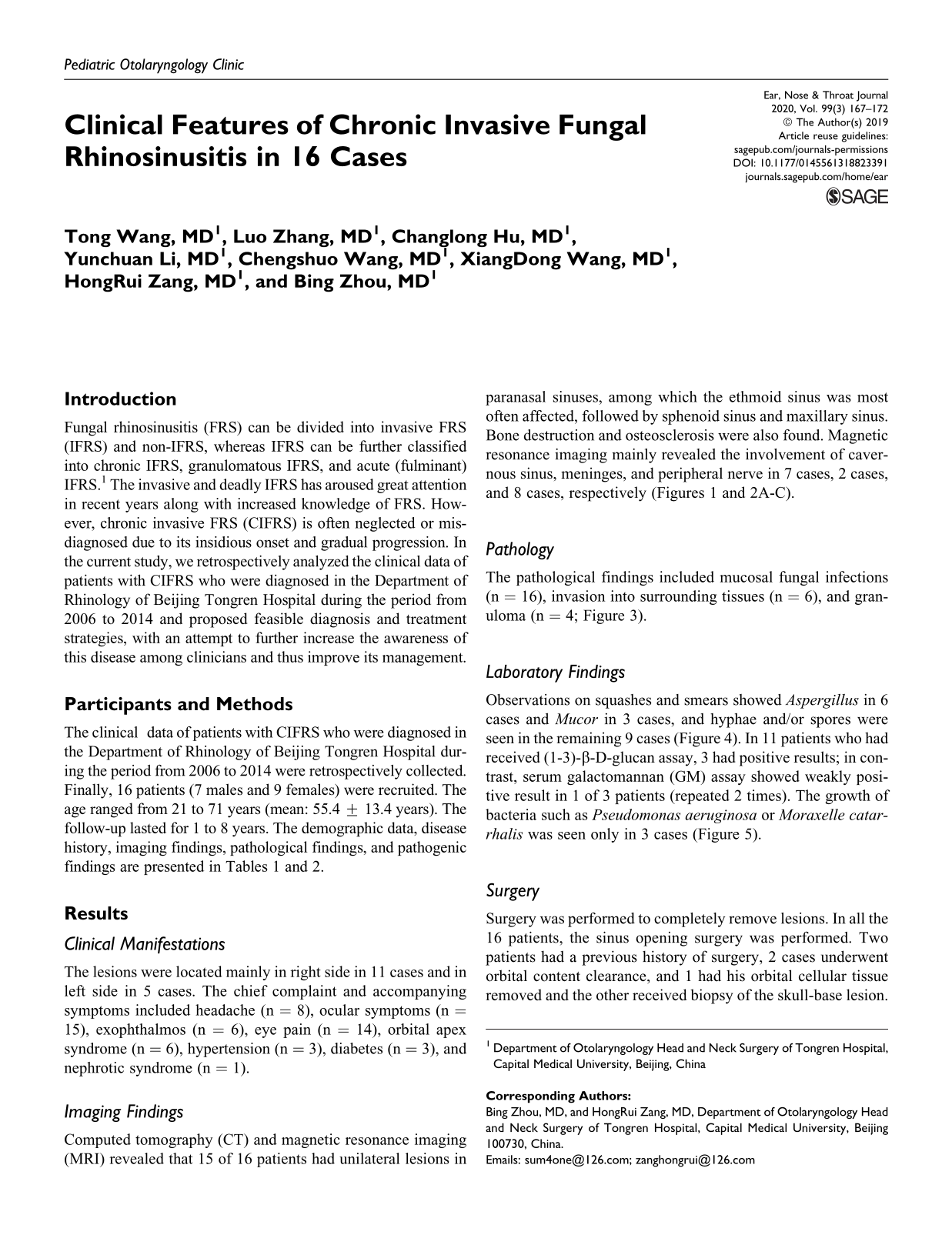
Computed Tomography and MRI Findings of 16 Patients With CIFRS.
Abbreviations: CIFRS, chronic invasive fungal rhinosinusitis; CT, computed tomography; MRI, magnetic resonance imaging; +, present; +, positive; −, negative.
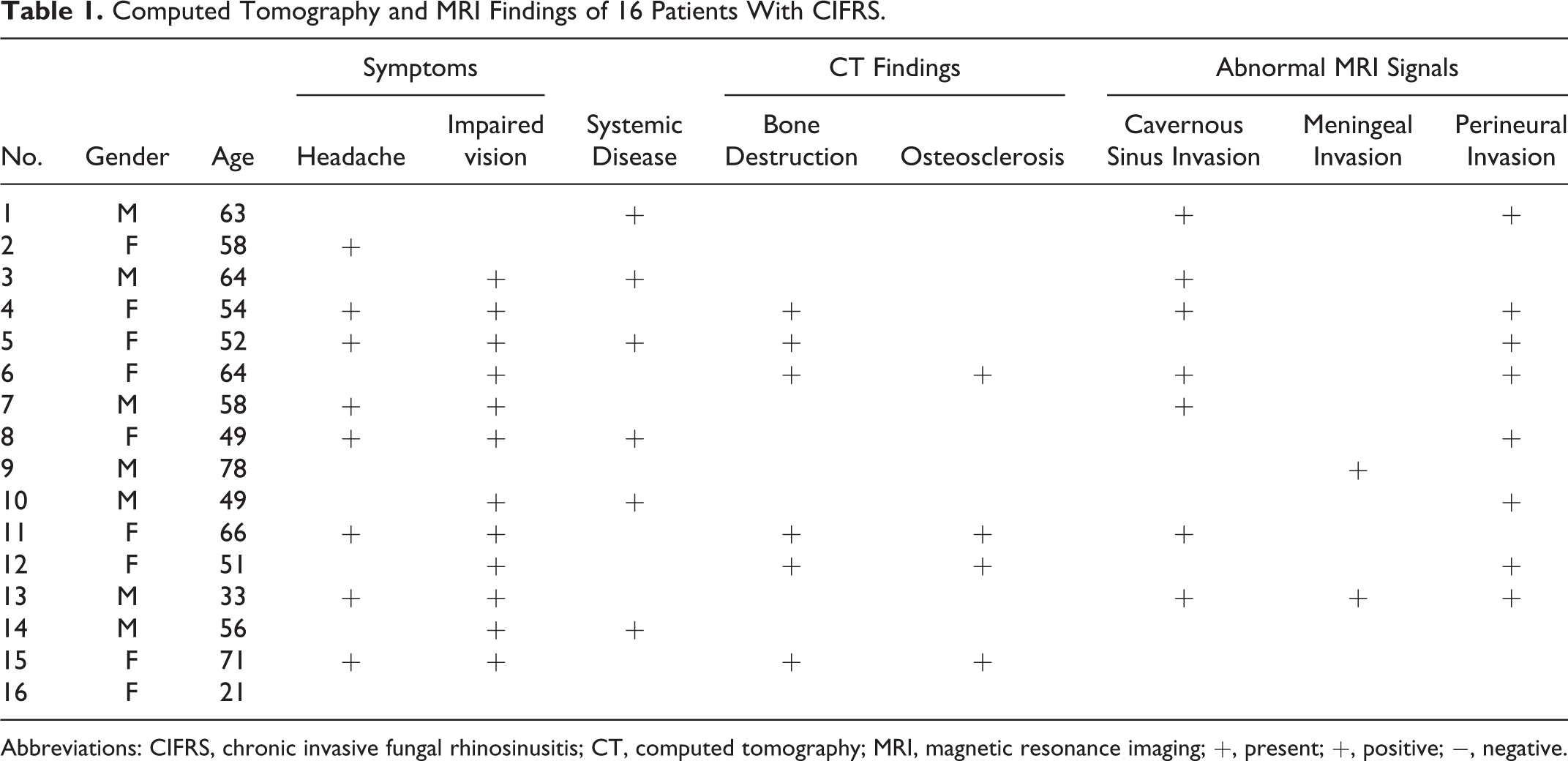
Pathology and Laboratory Tests Findings of 16 Patients With CIFRS.
Abbreviations: CIFRS, chronic invasive fungal Rhinosinusitis; GM, galactomannan; +, present; +, positive; −, negative.
Results
Clinical Manifestations
The lesions were located mainly in right side in 11 cases and in left side in 5 cases. The chief complaint and accompanying symptoms included headache (n = 8), ocular symptoms (n = 15), exophthalmos (n = 6), eye pain (n = 14), orbital apex syndrome (n = 6), hypertension (n = 3), diabetes (n = 3), and nephrotic syndrome (n = 1).
Imaging Findings
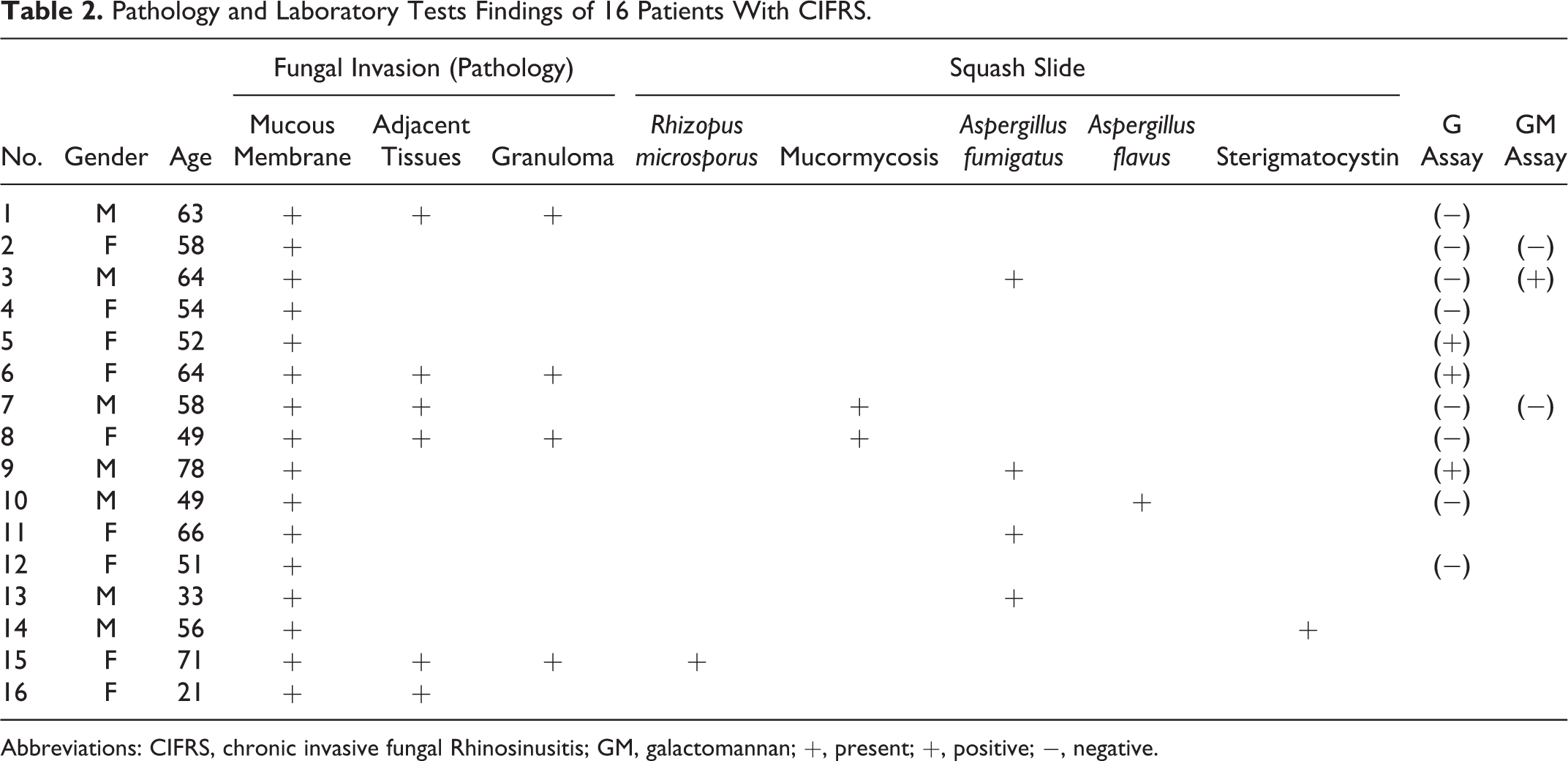
Computed tomography (CT) and magnetic resonance imaging (MRI) revealed that 15 of 16 patients had unilateral lesions in paranasal sinuses, among which the ethmoid sinus was most often affected, followed by sphenoid sinus and maxillary sinus. Bone destruction and osteosclerosis were also found. Magnetic resonance imaging mainly revealed the involvement of cavernous sinus, meninges, and peripheral nerve in 7 cases, 2 cases, and 8 cases, respectively (Figures 1 and 2A-C).

The ethmoid sinusitis in computed tomography (CT) scan of one patient with CIFS.
A, T1WI(T1 weighted image, T1WI) image of magnetic resonance imaging (MRI) in one patient with CIFS. B, T2WI(T2 weighted image, T2WI) image of MRI in the same section of the patient. C, T1WI enhanced image of MRI in the same section of the patient.
Pathology
The pathological findings included mucosal fungal infections (n = 16), invasion into surrounding tissues (n = 6), and granuloma (n = 4; Figure 3).
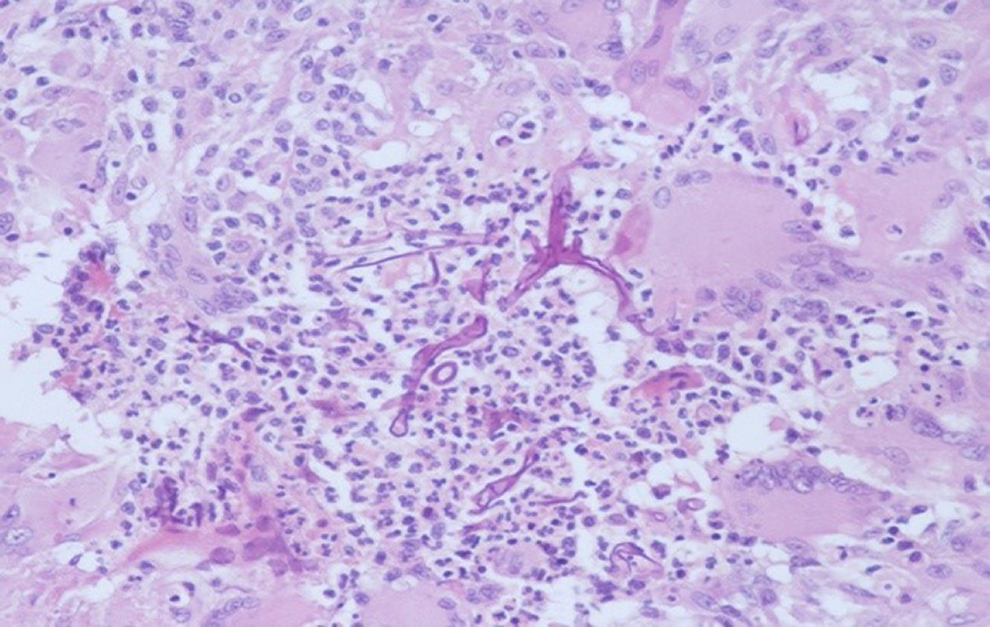
Fungal tissue found in pathological tissue section.
Laboratory Findings
Observations on squashes and smears showed Aspergillus in 6 cases and Mucor in 3 cases, and hyphae and/or spores were seen in the remaining 9 cases (Figure 4). In 11 patients who had received (1-3)-β-D-glucan assay, 3 had positive results; in contrast, serum galactomannan (GM) assay showed weakly positive result in 1 of 3 patients (repeated 2 times). The growth of bacteria such as Pseudomonas aeruginosa or Moraxelle catarrhalis was seen only in 3 cases (Figure 5).
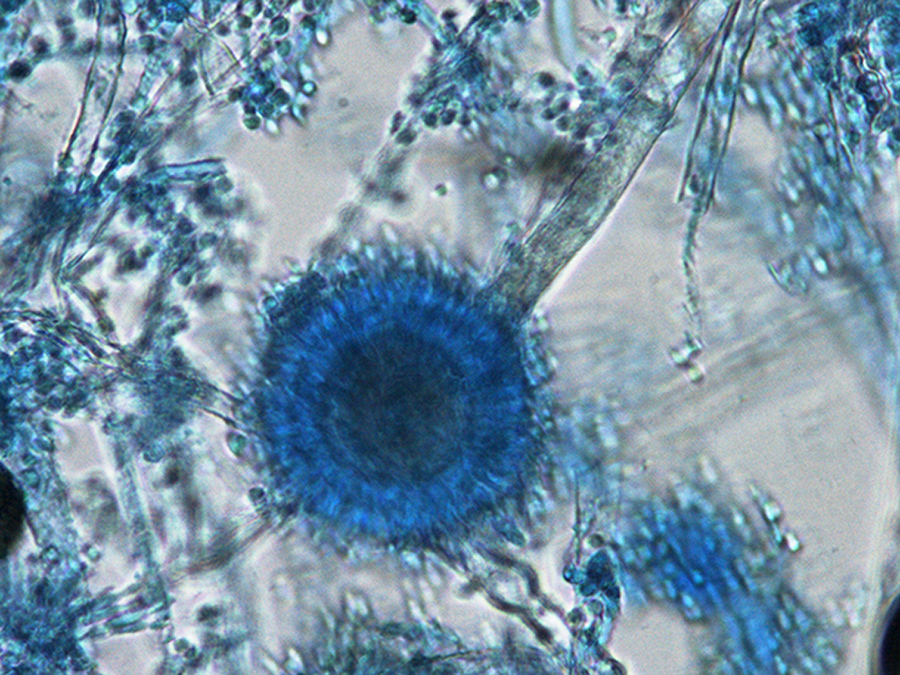
A fungal mycelium or spores found in exudate smear.
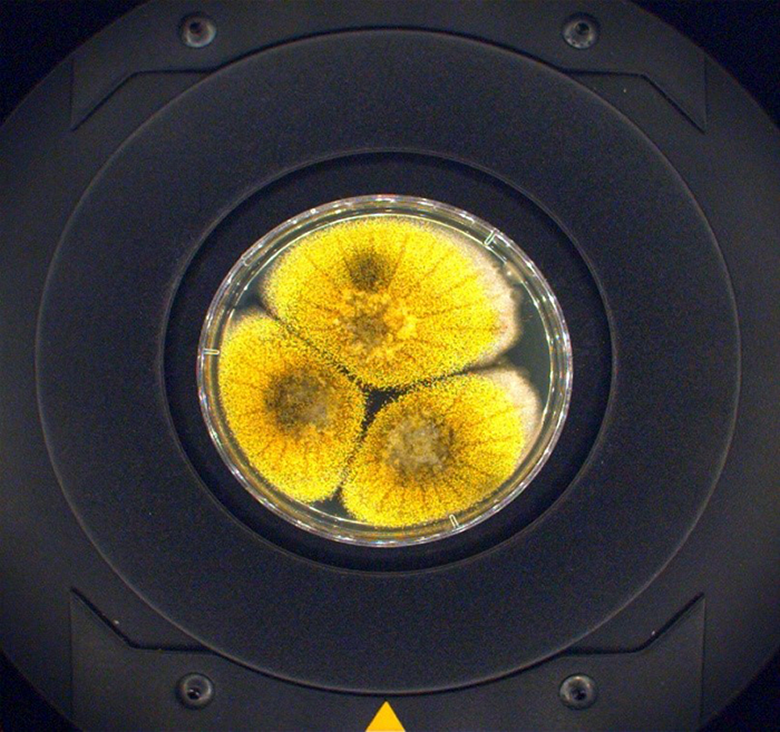
The positive fungal culture of one patient with CIFS.
Surgery
Surgery was performed to completely remove lesions. In all the 16 patients, the sinus opening surgery was performed. Two patients had a previous history of surgery, 2 cases underwent orbital content clearance, and 1 had his orbital cellular tissue removed and the other received biopsy of the skull-base lesion.
Follow-Up
All the 16 patients were followed up. After the surgery, antifungal therapy was applied in 10 of 16 patients, among whom 8 were treated with amphotericin B and 2 with voriconazole. Nasal irrigation was performed in 5 cases. Although no relapse occurred in 9 patients, 4 patients died from relapse 3 to 17 months after surgery. Twelve patients had preoperative visual dysfunction, which was improved after surgery in 4 patients.
Discussion
Invasive sinusitis is a new clinical entity firstly described by DeShazo et al 2 in 1997 and formally named by Stringer and Ryan 3 in 2000. It is featured by the gradual spread of fungal infection into surrounding structures and tissues, which may last at least one month. In its early stage, the fungal invasion is often localized within the mucosa and bony wall of one single paranasal sinus. Thus, it may gradually invade the adjacent paranasal sinuses and nasal cavity, although the symptoms are not obvious. In the later stages, the lesion can invade adjacent structures and tissues such as orbit and skull base. Based on the morphological features of the lesions in paranasal sinuses, it can be further divided into granulomatous and nongranulomatous types. Chronic IFRS is clinically featured by its insidious onset and gradual progression. In its early stage, it may be manifested as bloody nose or relatively severe headache. It may be accompanied by diabetes and leukemia, or the patients may have a history of long-term systemic glucocorticoid use. If diagnosed early, it can be cured in most cases, with very few relapses. The advanced CIFRS is more difficult to treat, with high risk of relapse and poor prognosis. The most common pathogen of CIFRS is Aspergillus, but the disease can also be caused by Mucorales, chain lattice such as Pseudomonas, Altemarias spp, and Candida spp. Once the invasive infection spreads to the intraorbital structures, the orbital bone can be eroded, which can be manifested as unilateral exophthalmoses, displacement of eyeball, superior orbital fissure syndrome, or orbital apex syndrome, which may lead to visual impairment. 1 Notably, a large proportion of patients in our series had eye symptoms.
Imaging Features
The typical CT findings of chronic invasive sinusitis include unevenly increased density of soft tissues in single or multiple paranasal sinuses, swelling, destruction, or even defect of the bones of the involved sinuses (especially in maxillary sinus). Varying degrees of hyperplasia and hardening of the stump and adjacent bones may also exist. The sinus cavity was filled with soft tissue shadows, which had irregular shapes and relatively even densities. Calcification is rarely seen. Typically, the lesion is often accompanied by peripheral obstructive inflammation of the paranasal sinuses, although it is difficult to distinguish these 2 conditions under CT. The lesion can easily spread to surrounding structures, mainly the orbital apex and/or the cavernous sinus but can also include meninges, pterygopalatine fossa, infratemporal fossa, nasopharynx, and palatum durum. 4 In our series, ethmoid sinus (n = 9) was the most commonly affected paranasal sinus, followed by sphenoid sinus (n = 8). The vast majority of the patients had unilateral paranasal sinus involvement, and only 1 patient had bilateral involvement. Bone destruction was found in 4 cases and bone hardening in 2 cases. Unevenly increased density of soft tissues in single or multiple paranasal sinuses, irregular bone destruction, and bone hardening may be the typical manifestations of chronic invasive sinusitis. The lesion may show equal signal on MRI T1WI (T1weighted image, T1WI); however, its signal may vary on MRI T2WI (T2weighted image, T2WI) and is related to disease course: it often shows high signal in the early stage but mainly low signal in later stages (typically uneven). The peripheral obstructive inflammation shows low or equal signal on T1WI and significantly high signal on T2WI, and its edge is remarkably enhanced after enhancement; thus, it can be easily differentiated from chronic invasive sinusitis. Perineural invasion of CIFRS can occur in an antegrade or retrograde manner, 5 thus causing clinical symptoms accordingly. Enhanced MRI can clearly reveal such change, with enhancement with fat-suppressed fast sequences being the optimal options. Compared with CT, MRI can more clearly reveal the scope of the lesion; in particular, it can accurately display the lesions in the orbital apex, cavernous sinus, brain parenchyma, meninges, and pterygopalatine fossa, which are enhanced on enhanced MRT1WI. In our series, MRI clearly revealed changes in cavernous sinus (n = 7), changes in orbital apex, pterygopalatine fossa, and infratemporal fossa (n = 8), and meningeal change in brain parenchyma (n = 2). The typical MRI findings included enhanced signals reflecting bone cracks and canal expansion along the nerves; meanwhile, the signals of adipose tissues in normal sites were weakened or disappeared. Most lesions can be diagnosed based on changes in bones and signals, along with relatively long disease histories and relatively mild clinical manifestations. However, histopathologic confirmation of diagnosis is essential. 6
Histopathological Features
Histopathological examinations of fungi mainly include hematoxylin-eosin staining (HE) staining, silver staining, PAS method, gomori’s methenamine silver nitrate stain (GMS) method, Fontana Masson silver method, and immunofluorescence assay. HE staining and histochemical staining: the main pathological features of invasive fungal disease include coagulative necrosis of tissues, chronic suppurative granulomatous inflammation, vasculitis secondary to fungal infections, purulent inflammation, and chronic nonspecific inflammation. Mycelium, usually in the cross section, may be occasionally seen in necrotic tissues under transmission electron microscope. Fungi have a thick outer membrane, showing homogeneous structures with high electron density. Fungal cell walls have a double bilayer membrane. Inside the fungal cells, the nuclei and organelles dissolved and disappeared, showing vacuolization-like appearance. Around the fungi were cellular debris resulting from tissue necrosis and disintegration. 7 The acute fulminant lesions mainly include coagulative necrosis and mycotic vasculitis, but can also be accompanied by pyogenic granuloma. The chronic invasive type mainly includes chronic suppurative granulomatous inflammation, which can often be accompanied by chronic nonspecific inflammation, whereas coagulative necrosis and mycotic vasculitis can also be observed in some cases. Coagulative necrosis and deformation often mark the rapid progression of the disease. Granulomatous reaction caused by fungi often results from chronic immune response and is also a histological feature of chronic invasive fungal disease. 8 In our series, 4 of 16 cases had granulomatous reaction. Mycotic vasculitis was also found, during which the hyphae of Mucorales and Aspergillus invade the small vascular walls and small arteries, leading to swelling of vascular endothelial cells, intimal thickening, luminal narrowing, and even luminal occlusion or fungal embolism. In our series, pathology showed that 3 of 16 cases had fungal invasion of the ipsilateral orbit, during which the fungi invaded the extrascleral connective tissue and the optic nerve.
Since CIFRS is typically caused by Mucorales and Aspergillus. The Mucorales are more invasive and often cause acute invasion and massive tissue necrosis; in contrast, the Aspergillus invades tissues in a slower pace, clinically manifested mainly by chronic invasion and microscopically mainly by granuloma. 9
During the histopathological diagnosis, techniques such as polymerase chain reaction combined with reverse line blotting (PCR/RLB) 10 and UC5B antibody (mucin 5b) are also used. 11
Laboratory Findings
Nasal secretions were harvested in the first physical examination for microbial culture, and meanwhile local mucosal and bone tissues were collected for pathological tests. Fungi can be detected several hours after smear preparation; however, it is difficult to identify the specific fungal species. In our series, hyphae or spores were detected in secretion smears in all 16 patients, among whom Aspergillus was identified in 6 and Mucorales in 3. The secretion smears had a success rate in detecting fungi; however, the growth of fungi was seen only in 3 cases, which might be attributed to the fact that the growth of the accompanying bacteria suppressed fungal proliferation.
The (1-3)-Beta-
Treatment of CIFRS
Surgery is the mainstream treatment for CIFRS. 14 It is important to completely remove lesions such as polyps, mucosal edema, and retention within the sinus cavities, eliminate abnormal structures (eg, concha bullosa, paradoxical middle turbinate, hypertrophy of uncinate process/ethmoid bulla, and deviation of nasal septum) that affect the drainage of nasal cavity and paranasal sinuses, and restore the drainage of nasal cavity and paranasal sinuses. An endoscopic nasal surgery can completely remove the lesions, establish adequate ventilation and long-term drainage channel in the paranasal sinuses, and thoroughly change the microenvironment where the fungi exists. 15 A second endoscopic nasal surgery may be performed in patients with relapse to get rid of the lesions. For patients with eye symptoms, ophthalmologic examinations should be performed as soon as possible. Computed tomography and MRI may be performed. Surgery shall be performed to relieve inflammation/edema and remove necrotic tissues, during which the optic nerves should be carefully protected. 16
Surgical treatment
Debridement of paranasal sinuses shall be performed in patients with CIFRS. Caseous exudates of different colors and necrotic tissues can be seen during endoscopic sinus surgery. After the lesions within the nasal cavity and paranasal sinuses are completely removed, extensive resection of the involved mucosa and bony walls of the sinuses should be performed based on the scope of the lesions. A traditional surgery or endoscopic surgery may be selected based on the scope of the lesions. 17
Medical therapies
Antifungal drugs must be applied postoperatively. Two commonly used drugs are itraconazole and amphotericin B, whereas other drugs such as clotrimazole, nystatin, and posaconazole can also play a role. Itraconazole is effective for Aspergillus, with little side effects. Amphotericin B is a broad-spectrum antifungal agent for Cryptococcus, Histoplasma, Blastomyces, Paracoccidioides, Coccidioides, Aspergillus, Mucorales, and some Candida species. It is especially effective for CIFRS, but with severe side effects. Voriconazole is commonly used, with a loading dose (day 1) of intravenous (IV) 6 mg/kg or oral 400 mg Q12 hours; the maintainence dose is IV drip infusion 4 mg/kg or oral 200 mg Q12 hours. Alternately, amphotericin B liposome can also be used at a loading dose of IV drip infusion 0.1 mg/kg/d; on the next day, the dose can be increased to 0.25 to 0.5 mg/kg/d and then gradually increased to 1 to 3 mg/kg/d. The total dose will be 1 to 5 g. It is recommended that the oral administration of antifungal drugs should last 3 to 6 months, during which the routine blood test and tests for liver/kidney functions should be performed regularly. Patients will need to have antifungal treatment for at least 2 weeks, and the total treatment course shall be 3 to 6 months. The treatment should not be stopped until the clinical symptoms and signs are dissolved, the potential infection factors are eliminated, the imaging modes reveal normal findings, and the results from the culture are negative.
Other treatments
Antifungal nasal lavage is often applied after surgery in patients with CIFRS. In our center, one vial (5 mg) of amphotericin B is diluted with 500 mL of normal saline; 2 mL of the mixture is placed in 500 mL of normal saline for each lavage. It has also been proposed that intermittent oxygen inhalation should be provided in patients with advanced chronic or acute invasive fungal sinusitis, during which the use of antibiotics and immunosuppressive agents should be stopped, along with efforts to improve the general conditions. Control of primary diseases and systemic supportive therapies are also important treatments.
Here are some key points during the diagnosis and treatment of CIFRS: (a) The suspected cases must be timely identified. For immunocompromised patients with pain or bleeding in nasal cavity and paranasal sinuses, swelling of maxillofacial tissues, visual impairment, headache, poorly controlled diabetes, and/or long-term use of immunosuppressive agents (eg, for leukemia), an early diagnosis should be made, during which disease history and physical examinations are particularly important. Culture of local secretions and tissues should be performed to identify the pathogens and the invasive changes should be confirmed by pathology. (b) The underlying disease and its complications should be controlled, and supportive measures should be provided. Multidisciplinary consultations should be arranged since the disease may involve multiple systems and cause relevant dysfunction. Thus, specialists from the departments of internal medicine, neurology, ophthalmology, radiology, laboratory, and pathology should be invited to help confirm the diagnosis and propose multidisciplinary treatment protocols. (c) Tailored medications and nasal irrigation. Long-term antifungal treatment should be carried out after surgery. For instance, amphotericin B liposome is used firstly; after the total dose is reached, oral itraconazole is used instead, with a total treatment course of 3 to 6 months. (d) Radical surgical debridement. The surgical principle is to remove all the accessible necrotic and suspicious tissues including tissues in nasal cavity and paranasal sinuses, orbital contents, and necrotic bone tissues (eg, maxillary bone). (e) Follow-up: Endoscopic examination of the nasal cavities can be performed regularly and the cavities should be cleaned. If any suspicious tissue is found, the secretions of the operated cavity should be collected for fungal culture. If necessary, mucosal and bone tissues can be collected for pathological observation to identify any fungal infiltration. Computed tomography and MRI may be performed to find the lesions. Thus, the prognosis may be improved.
In summary, early detection and early diagnosis are essential for CIFRS, whereas surgery and medications are key to treatment success. Intracranial invasion is particularly dangerous. Chronic invasive FRS is featured by insidious onset and poor prognosis, and thus adequate attention must be paid to this disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.