
Abstract
Superior laryngeal nerve neuralgia (SLNN) is an anterior neck pain syndrome that is underrecognized and, as a result, is often misdiagnosed. We present a series of patients who were diagnosed with and subsequently treated for SLNN. Nineteen patients were treated with oral nonsteroidal anti-inflammatory drugs (NSAIDs) and/or a therapeutic neck injection with 2% lidocaine and 40% triamcinolone acetonide. All patients completed a visual analog scale (VAS) to rate the level of pain before and after treatment. Four patients rated their pain as mild, 14 as moderate, and 1 as severe according to the VAS. Of the 19 patients, 8 chose to proceed with a 2-week course of NSAIDs and only 1 of them had complete resolution of their symptoms. A total of 18 patients underwent therapeutic neck injections, with a complete response to injection therapy in 10 patients. Five patients described a minimal residual foreign body sensation and 3 patients complained of mild residual pain. In this study, we found that therapeutic neck injections are effective not only in confirming the diagnosis but also in treating pain.
Introduction
Patients frequently present to the otolaryngology clinic with neck pain as their chief complaint or as a major component of a different chief complaint. Anterior neck pain is defined as pain anterior to the sternocleidomastoid muscle while posterior neck pain is defined as pain posterior to this structure. Posterior neck pain often can be secondary to musculoskeletal issues along the cervical spine and will not be discussed in this manuscript.
The differential diagnosis of anterior neck pain is very broad, including infectious, inflammatory, functional, congenital, and neoplastic etiologies. Anterior neck pain syndromes are not well understood and therefore are often overlooked or misdiagnosed.
The socioeconomic impact of diagnosis and management of anterior neck pain can be significant. Patients will often see multiple physicians over several visits, and in some cases, this may lead to unnecessary imaging, treatment, or referrals that increase cost to the patient and add to their frustration.
There are several anterior neck pain syndromes that have been well described in the literature, yet they are often not considered in the differential diagnosis. In this case series, we report on 19 patients with superior laryngeal nerve neuralgia (SLNN). Clinical characteristics, diagnostic workup, and treatment options are presented and compared to other less-known anterior neck pain syndromes.
Patients and Methods
Ethical Considerations
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all participants. Approval for this study was obtained from the institutional review board at University Hospitals Cleveland Medical Center.
Patients
Charts of 19 patients diagnosed with SLNN between 2014 and 2017 were reviewed. All patients completed a validated visual analog scale (VAS) on a 100-mm horizontal line to indicate their pain, with 0 mm reflecting no pain and 100 mm the most severe pain. The VAS ratings of 0 to 4 mm were considered no pain, 5 to 44 mm as mild pain, 45 to 74 mm as moderate pain, and 75 to 100 mm as severe pain. A 33-mm change on the VAS was defined as a change in pain that was meaningful from the patient’s perspective. 1
Diagnosis and Treatment
Diagnosis of SLNN was made by the patient’s history, head and neck examination with careful palpation and, in some cases, imaging, which was obtained to rule out other pathologies. All 19 patients who were diagnosed with SLNN were offered treatment. They could choose between a 2-week course of oral ibuprofen (600 mg 4 times a day) or a neck injection therapy with of a mixture of 2% lidocaine and 40% triamcinolone acetonide into the foramen area of the SLN along the posterior thyrohyoid ligament.
Neck Injection for Neuralgia of the SLN
The neck is positioned in slight extension and turned to the contralateral side. The skin is disinfected with alcohol or betadine. The examiner places his or her hand around the patient’s larynx to rotate and push the laryngeal complex to the ipsilateral side away from the carotid artery and more superficially. This allows the examiner to better appreciate landmarks around the entry point of the SLN, including the greater horn, the hyoid bone, and superior thyroid cornu. Ultrasound-guided injections can be considered in cases in which landmarks are difficult to palpate and to avoid accidental puncture of the carotid artery.
A half-and-half mixture consisting of 2% lidocaine and 40% triamcinolone acetonide is injected by advancing the needle toward the foramen, located just anterior to the superior thyroid cornu, which can be palpated with the needle tip if necessary to confirm the correct location (Figure 1). The thyroid membrane can usually be palpated with the needle tip indicating the correct depth. A volume of 2 mL is infiltrated around the SLN entry point. If the injection was placed correctly, patients will report temporary numbness of the ipsilateral throat.
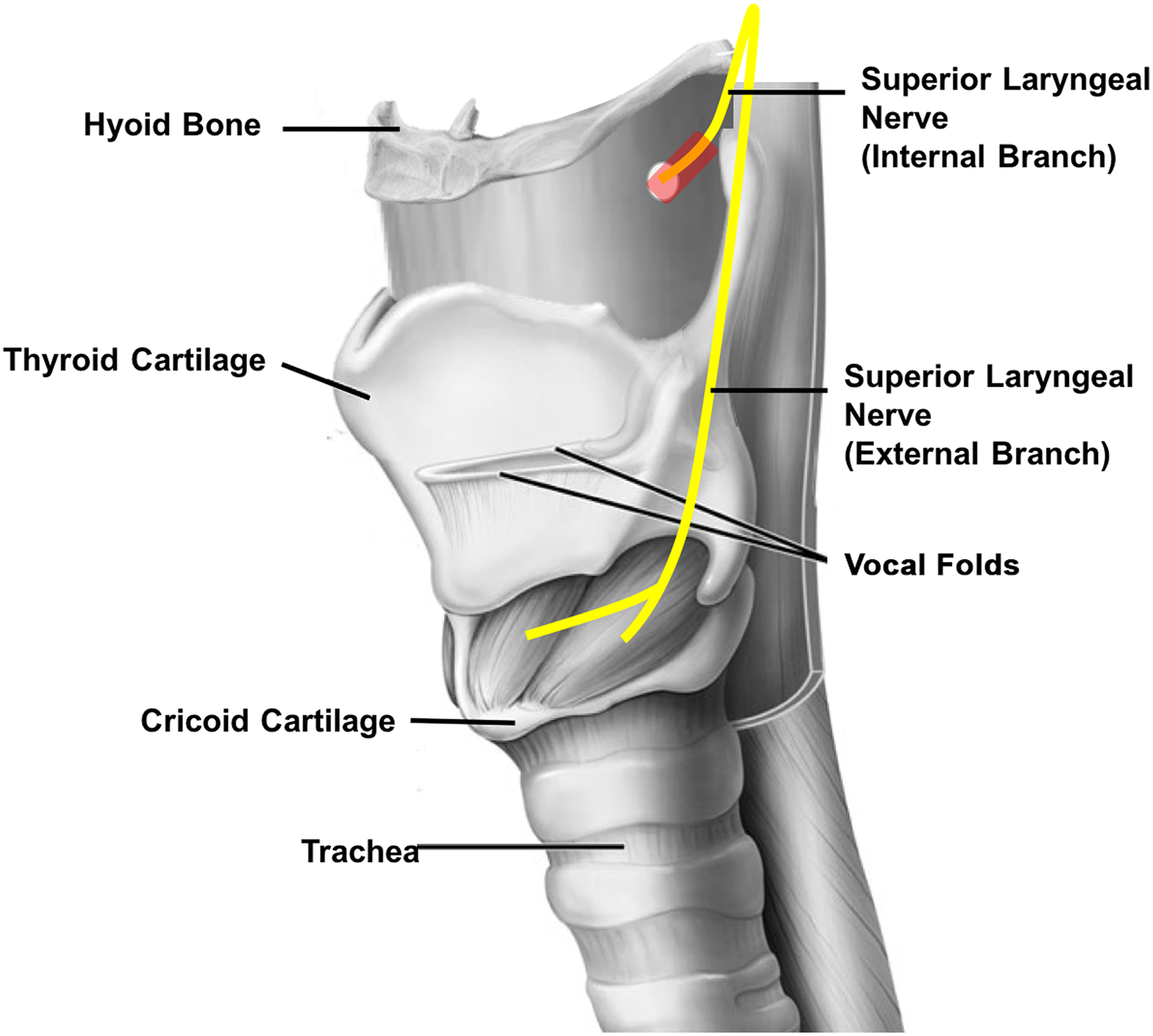
Injection therapy of the superior laryngeal nerve neuralgia with a mixture of 2% lidocaine and 40% triamcinolone acetenoide. The superior laryngeal nerve is located along the posterior thyrohyoid space. The area of inflammation is highlighted in red. The superior thyroid cornu is palpated with the needle tip while the medication is infiltrated up to 1 cm farther anteriorly, depositing approximately 2 mL lateral to the thyrohyoid membrane, which can usually be palpated with the needle tip. Image adapted from the website of the National Cancer Institute (https://www.cancer.gov).
Results
A total of 19 patients with SLNN sought medical care for anterior neck pain. There were 10 female and 9 male patients ranging from 24 to 75 years of age with a mean age of 46.5 years. In 10 patients, the pain was on the left side and in 9 patients on the right side. Duration of pain before presentation to our clinic varied from 3 weeks to 12 months. Follow-up ranged from 6 to 19 months.
Four patients rated their pain as mild, 14 patients as moderate, and 1 patient as severe. Twelve patients described their neck pain as sharp, 6 described a radiating pain to the ipsilateral ear, 7 described odynophagia, and 1 complained about increased pain with head turn. All 19 patients were successfully treated for SLNN and needed no further intervention. Of the 19 patients, 8 decided to proceed with a 2-week course of ibuprofen; 11 declined nonsteroidal anti-inflammatory drug (NSAID) treatment and opted to proceed directly with neck injection.
Only 1 patient, who had presented with very mild pain, achieved complete pain resolution with NSAIDs; the other 7 patients proceeded with injection therapy. A total of 18 patients underwent between 1 and 3 neck injections for SLNN. All patients had a meaningful improvement of their pain after treatment was completed. Five patients required 1 injection, 10 patients a series of 2 injections, and 3 patients a total of 3 injections to treat their pain.
Ten patients had complete pain relief from injection therapy, and 5 noted a mild residual foreign body sensation but no pain. Four patients complained of mild residual pain at the end of their treatment course but were not interested in further intervention due to tolerability of the remaining mild discomfort.
Discussion
Anterior neck pain syndromes, including SLNN, are poorly recognized by physicians and, therefore, delayed diagnosis and inadequate treatment are common. In some cases, SLNN can be difficult to differentiate from other conditions that will be reviewed in this article.
The SLNN was first described in 1866 by Tobold. 2 It is characterized by paroxysmal, unilateral pain originating from the posterolateral thyrohyoid space often radiating along the neck. 2 The etiology of SLNN is unclear, but trauma, infection, and inflammation are all possible mechanisms that have been considered. 3,4 Only a few small case studies on SLNN have been described in the literature over the past few years. 5,6 We have presented a series of 19 patients diagnosed and treated for SLNN.
A clear understanding of the SLN and the surrounding anatomy of the anterior neck is critical. The SLN splits into an external motor and an internal sensory branch. The internal branch, which is involved in SLNN, will travel through the posterior thyrohyoid ligament deep to the thyrohyoid muscle, accompanied by the superior laryngeal artery.
The anatomic course of the SLN has been studied, and in over 80% of cases, the SLN penetrated the thyrohyoid membrane 0.1 to 0.9 cm from the posterior border of the thyrohyoid muscle and 0.1 to 1.2 cm from the superior border of the thyroid cartilage. 7 This small foramen serves as an external trigger point for pain.
In our series, SLNN was a clinical diagnosis based on the history and physical examination, with special attention to the location and distribution of the patient’s reported neck pain. Imaging is usually not necessary to diagnose SLNN and is only helpful to rule out other causes if the clinical picture is not straightforward.
Pain associated with SLNN is located in the area of the SLN traversing the posterior thyrohyoid membrane. The SLNN pain is often localized but also may radiate superiorly or inferiorly along the anterolateral neck. Anesthetizing the larynx with infiltration of local anesthetic around the entry point of the SLN serves as a diagnostic as well as a therapeutic procedure to confirm SLNN. 6
In our series, 9 patients reported localized pain while 6 noted radiating pain. Movement and stretching of the nerve with head movement or swallowing may exacerbate the pain. Of the 19 patients, 7 experienced odynophagia. Straining or projecting the voice can also serve as a trigger for pain in some patients.
Several other conditions can imitate SLNN and should be included in the differential diagnosis of anterior neck pain. Up to one-fourth of patients with rheumatoid arthritis will have laryngeal symptoms due to involvement of the cricoarytenoid joint. Foreign body sensation, throat pain, referred otalgia, and hoarseness are common. 8 Laryngoscopy on these rheumatoid arthritis patients will reveal an erythematous and swollen arytenoid, sometimes associated with hypomobility of the vocal fold.
Carotidynia also presents with unilateral neck pain, but unlike SLNN, point tenderness is located more lateral over the carotid bifurcation. We have found that rotating the larynx, as described in “Methods” section, will separate these 2 areas to differentiate SLNN from carotidynia. The etiology of carotidynia is controversial, and some authors have even grouped it with a form of vasculitis due to the presence of focal eccentric thickening of the carotid wall. 9
Eagle syndrome, which also needs to be considered in the differential diagnosis for SLNN, is secondary to an elongated styloid process or calcified stylohyoid ligament. Patients will often present with throat pain, odynophagia, dysphagia, and anterolateral neck pain. Facial or retro-orbital pain, syncopal events, and headache have been reported in the context of Eagle syndrome but are rather uncommon. Palpation of the tonsillar fossa is a trigger point that will help in making the diagnosis of Eagle syndrome. Patients often have a history of tonsillectomy, which might have caused scarring of the pharyngeal wall involving the peristyloid tissue and glossopharyngeal nerve. 10 A transoral injection with lidocaine into the peristyloid area can help confirm the diagnosis.
There are multiple muscular attachments to the hyoid bone contributing to speech and swallowing function. These include the prelaryngeal strap muscles, the digastric muscle, and stylohyoid muscle. All of these can be involved in anterior neck pain, which can imitate or even be associated with SLNN. Muscular pain associated with muscle tension dysphonia (MTD) is common and often can be diagnosed based on history and physical examination alone. Patients will often describe voice changes with strain and vocal fatigue.
In patients with MTD, palpation of the prelaryngeal musculature may reveal bilateral tenderness, tightness, and nodularity, often found at the level of the anterior thyrohyoid space. The SLNN-associated pain is located farther posterior on the thyrohyoid membrane and is usually only unilateral.
Differentiating MTD from SLNN can be quite difficult in some cases, as patients may present with a combination of MTD and SLNN. Flexible laryngoscopy can show excessive supraglottic squeeze or abnormal mucosal wave during phonation. Patients with MTD typically do not respond to injections, but rather to voice therapy or manual massage of the hyolaryngeal segment. In contrast, patients with SLNN will not respond to massage of the larynx.
Hyoid bone syndrome and superior thyroid cornu syndrome can present with symptoms similar to those of SLNN, including throat pain, odynophagia, and globus sensation. Hyoid bone syndrome is believed to be related to an insertion tendinitis or tendinosis of the muscular attachments to the hyoid bone. 11 Laryngoscopy commonly reveals hypopharyngeal indentation due to a prominent superior thyroid or hyoid cornu. Careful palpation of the greater cornu of the hyoid bone or thyroid cartilage will often reproduce symptoms, which may help to differentiate each syndrome.
In general, nerve pain is often challenging to manage because of the heterogeneity of its etiologies, symptoms, and underlying mechanisms. Baxter et al have suggested performing an incision of the thyrohyoid membrane to relax the inflamed SLN. 4 The SLNN is categorized as peripheral nerve pain. While trigeminal or glossopharyngeal neuralgia is often described as shooting pain, SLNN is usually described as a more constant and nagging pain that may radiate or worsen with swallowing or head turning.
Several treatment options have been proposed in the literature to manage SLNN. Carbamazepine has been used successfully in several cases. 12 Other authors have reported good outcome with injection of local anesthetic. 5 Local anesthetics are commonly injected to block local sensory signals and potentially decrease nerve sensitization. Interestingly, in a recently published Cochrane review, topical lidocaine was ineffective in treating neuropathic pain. 13
Some authors have proposed neuritis with local inflammation to be the underlying cause. In our experience, either oral or injection anti-inflammatory therapy should be strongly considered in cases of suspected SLNN to address the underlying neuritis. According to the patients’ treatment choice in our series, they were treated with NSAIDS and/or neck injection therapy consisting of a mixture of lidocaine and steroids. Of our 19 patients, 8 agreed to a trial of oral NSAIDs, but only 1 patient with mild pain reported adequate pain relief with NSAIDs. Injection therapy consisting of a mixture of lidocaine and triamcinolone acetonide was used to treat 18 of 19 patients, resulting in complete resolution of SLNN pain or improvement in pain to a VAS level categorized as mild.
All patients in this series were diagnosed with SLNN based on clinical examination, with pain over the entry point SLN and not the hyoid, thyroid, or tendon. 11 However, because of the close anatomic relationship, SLNN can easily be confused with or misdiagnosed as hyoid bone syndrome, superior thyroid cornu syndrome, or tendinitis. Steroid injection therapy into the area of the posterior thyrohyoid complex has been shown to be effective in all the previously mentioned conditions due to a likely underlying inflammation. Further research is therefore needed to prove that SLNN is truly a nerve-related pain syndrome.
Injection therapy with triamcinolone acetonide has been described as safe and effective for hyoid bone syndrome. Stern et al reported a complete response in 74% in their series of 83 patients. 14 More than half of their patients required at least 1 additional steroid injection, which is consistent with our results in 14 of our 18 patients requiring more than 1 neck injection.
Serial injections over several weeks were well tolerated, and our patients did not experience any side effects aside from acute pain when the injection was performed.
Conclusion
Although SLNN is an uncommon cause of anterior neck pain, it should be considered within the larger differential diagnosed for anterior neck pain. In our series, injection therapy was found to be effective in treating patients whose pain did not resolve with oral ibuprofen. In our opinion, neck injections for SLNN serve as a diagnostic and therapeutic intervention with low risk and should strongly be considered if SLNN is suspected. Further research will be needed to better understand and determine the most effective treatment approach for SLNN.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.