
Abstract
Medical malpractice is costly and disruptive, and it is important to prevent. We conducted a study with the objective to look at medical malpractice in robotic surgery overall, to evaluate reasons for litigation, and to comment on possible strategies to avoid litigation with transoral robotic surgery. We used the Westlaw computerized database to identify all state and federal verdict summaries in medical malpractice cases. We found 17 cases alleging malpractice that involved the use of robotic surgery. In all, the plaintiffs in 6 cases (35%) contended that an open rather than a robotic approach should have been used, 5 (29%) alleged negligent credentialing, 4 (24%) alleged training deficiencies, 2 (12%) alleged manufacturing problems, and 1 (6%) charged that robotic surgery should have been performed instead of open surgery (1 case involved two of these allegations). In 11 cases (65%), plaintiffs charged that robotic surgery contributed to an undesirable outcome, and in 6 cases (35%) they raised concerns about informed consent. In all, only 5 of the 17 lawsuits (29%) resulted in plaintiff verdicts or settlements; damages ranged from $95,000 to $7.5 million. We believe the courts should not play a major role in establishing safety guidelines for the introduction of new technology such as robotic surgery. Instead, training and credentialing guidelines should be established by appropriate national associations and societies to assist hospitals in doing so.
Introduction
New technologies and procedures frequently are added to the armamentarium of head and neck surgeons. The decision as to which procedures and which new technologies to embrace can be a confusing proposition given the conflicting goals of a manufacturer's representative to sell a device, our need for improved technology, and our obligation to keep healthcare costs down. Added to these conflicts is the aggressive malpractice environment in the United States and, most important, our primary obligation to quality care and patient safety.
The purpose of this article is to look at medical malpractice as it relates to robot-assisted resections. In evaluatingthe litigation involved in robotic surgery cases in general, we have endeavored to define the factors that were considered in bringing suit. We then evaluated the factors that might be important in terms of robotic surgery through the mouth via transoral robotic surgery (TORS). We planned this approach because TORS is still relatively new, and related medical malpractice trends have not yet been established. In general, however, robotic surgery has been around long enough that some precedents have been established.
In this article, we describe our attempt to use a litigation analysis tool to evaluate the safety and malpractice concerns relative to robotic surgery in general, and to present our findings in relation to TORS in the practice of head and neck oncology. We also extend ourthoughts about the efficacy of the tort system in evaluating new technologies, as well as some thoughts that might be helpful in preventing medical malpractice claims in the arena of new technologies.
Materials and methods
We used the Westlaw computerized database to evaluate medical malpractice claims associated with robotic surgery of any kind. Westlaw is a search tool that evaluates past lawsuits. It can be searched for specific phrases pertaining to disease types, anatomic sites, and types of procedures, such as robotic surgery. The information in the lawsuit database has been voluntarily submitted, and only those suits that progressed far enough to be registered in the public domain are included. Attorneys consider these suits to be informative in terms of both the likelihood of successful litigation and possible award amounts when considering potential litigation.
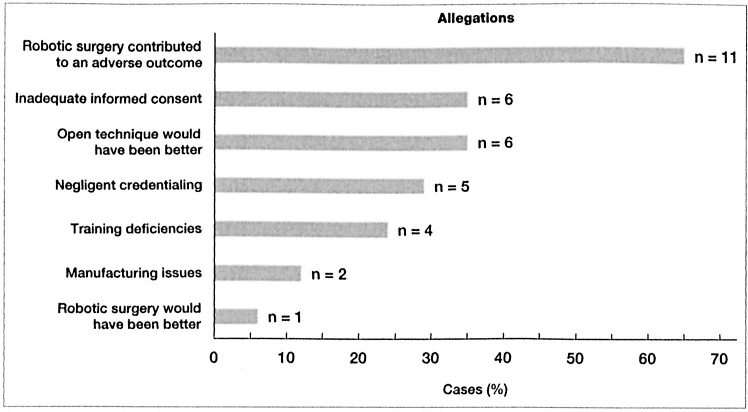
Figure. Chart quantifies the nature of the allegations in 17 malpractice lawsuits involving robotic surgery.
We have previously used this database to evaluate verdict summaries for various head and neck cancers, including those of the larynx, thyroid, oral cavity, and skin.1–4 For the current study, we employed the advanced search option to evaluate robotic surgery in general and TORS in particular.
Results
We searched the Westlaw data from 2005 through 2013 and identified 17 legal cases with verdict summaries that pertained to robot-assisted surgeries. We found no cases in which TORS was specified.
Of these 17 cases, 11 (65%) were concluded from 2011 through 2013. The 17 cases were filed in 13 different states. Most of the plaintiffs were male (n = 12; 71%), and just over half had cancer (n = 9; 53%).
These lawsuits involved a total of 27 defendants. In terms of specialty, 8 defendants (30%) were urologists, 6 (22%) were general surgeons, 6 were cardiothoracic surgeons, 5 (19%) were gynecologists, 1 (4%) was an orthopedic surgeon, and 1 was a neurosurgeon. In addition, a proctor or assistant was also sued in 5 cases.
In 11 of the 17 cases (65%), plaintiffs charged that robotic surgery contributed to an undesirable outcome, and in 6 cases (35%) they raised concerns about informed consent. Plaintiffs in 6 cases (35%) contended that an open rather than a robotic approach should have been used, 5 (29%) alleged negligent credentialing, 4 (24%) alleged training deficiencies, 2 (12%) alleged manufacturing problems, and 1 (6%) charged that robotic surgery should have been performed instead of open surgery (1 case involved two of these allegations) (figure).
Plaintiff verdicts or settlements occurred in only 5 cases (29%), and damages ranged from $95,000 to $7.5 million.
Discussion
Medical malpractice costs in the United States began rising in the early 1970s and they continue to escalate.5–7 Nationwide, malpractice costs have been estimated to exceed $55 billion annually. 7 This cost must be balanced against the positive aspects of the legal system. Proponents of our system argue that the threat of the tort system is an effective tool that encourages providers to be vigilant and careful. Critics argue that the system leads to the practice of defensive medicine and the overuse of tests and services. 8 Whether the legal system is a useful tool for vetting new technology is unknown.
In a recent article, Minami et al attempted to evaluate the impact of the medical malpractice environment on surgical quality and outcomes. 6 They failed to find any consistent data regarding the ability of malpractice liability to affect outcomes. Looming liability does, however, change physician behavior. According to a Jackson Healthcare poll (conducted by Gallup) of practicing U.S. physicians in 2009,73% admitted to ordering unnecessary tests because of the fear of litigation. 9 The estimated costs of these tests ranged from $650 billion to $850 billion.
In 2005, Studdert et al published a survey of defensive practices used by 824 emergency medicine physicians, orthopedic surgeons, neurosurgeons, and radiologists; they found that 93% reported practicing defensive medicine. 10 A survey of U.S. orthopedic surgeons published by Sethi et al in 2012 found that defensive imaging represented 19 to 24% of all imaging ordered. 11 In a 2007 report, Baicker et al analyzed data from the Medicare program and found an association between state malpractice liability indicators and decreased Medicare spending and malpractice costs, but there was no association with mortality. 12
As litigation pressures mount, some physicians avoid high-risk specialties or certain geographic areas, and others simply retire early.5,13 Access to healthcare in the United States has undoubtedly suffered in some areas because of this threat.
Is the tort system an effective deterrent to medical malpractice? Morris et al looked at the cases of 171 patients with a potential adverse event and a risk-management claim file and found no link between tort system deterrence and the reduction of adverse events. 14 In analyzing many of these reports, Minami wrote, “[T]hough there is evidence that medical malpractice liability influences physicians’ clinical choices, there is little to support the theory that the threat of medical litigation improves physician adherence to quality care indicators or improves patient outcomes.” 6
Nevertheless, errors do occur, of course, but most physicians are understandably afraid to fully/completely disclose errors for fear of litigation, which limits the effectiveness of the tort system in preventing malpractice.15–17 Moreover, the tort system takes an average of 44 months to resolve a case, further limiting its efficiency as a preventive or safety tool. 18 Finally, malpractice claims account for only 0.2% of all hospital discharges, and less than 2% of presumed true adverse events ever result in a claim against a physician. 15
Because the vast majority of events never enter the legal system, it is unrealistic to think that our current tort system would have much impact on the quality of care or the prevention of errors. In fact, it seems unreasonable to think that the tort system can be relied on to ensure patient safety.
A rapid growth in robot-assisted surgeries has occurred in a number of specialties, including head and neck surgical oncology. From 2007 to 2009, the number of da Vinci Surgical Systems (Intuitive Surgical; Sunnyvale, Calif.) installed in the United States grew from 800 to around 1.400. 19 Outside the United States, the number doubled from 200 to 400. 19
Evaluations of the costs, training, credentialing, proctoring, and medicolegal risks associated with robot-assisted surgery have been published.19–23 Surveys of surgeons reported as recently as 2013 have revealed that most (87%) were trained through industry-sponsored programs. 24 Analyses of outcomes and the costs of care associated with TORS for the treatment of oropharyngeal cancers have yielded some promising data in terms of lower rates of gastrostomy and tracheotomy tube placement, as well as shorter hospital stays. 25 However, complication rates with TORS are relatively high (as high as 10%). 24
Despite the higher complication rate, the expansion of TORS has not resulted in a corresponding increase in malpractice suits, which suggests that the procedure is generally safe. Guidelines for various robotic procedures and sites will need to be developed, and no standard credentialing system exists. Credentialing for TORS in our community (Omaha, Neb.) varies among the different hospitals, which develop their own procedures.
According to Intuitive Surgical, the manufacturer of the da Vinci Surgical System, a surgeon needs a minimum of only 20 completed cases to qualify to serve as a proctor. 20 Simulators, proctoring, preceptoring, and remote proctoring have been evaluated. 20 A large percentage (65% in 2008) of radical prostatectomies are performed with these minimally invasive robotic procedures, but head and neck procedures are not yet as common. 26 Training models for TORS that take surgeons from the laboratory to the patient have shown promise in multiple metrics. 26 These models are designed to decrease the workload of mentors and to provide objective feedback for trainees.
Training must be flexible and individualized to allow participants to progress at their own rate. 27 Training can be achieved through mini-residencies and simulators where available and by proctors and preceptors. Repetitive practice in a safe environment such as a simulator would be ideal, but the notion that a more experienced assistant could take over an operation if necessary is also appealing. In the future, perhaps remote proctoring will become available and be used much in the way that telemedicine is. 20 This would allow a surgeon to perform a procedure in his or her own hospital while the proctor observes remotely.
A failure to disclose training levels to patients may raise concerns in terms of informed consent should a lawsuit be filed. 21 Consent issues should be addressed from the start with a frank discussion and clear explanation of the limitations of training and the role of proctors and preceptors. This should include a discussion of the pros and cons of both robotic and open surgeries. The written form of consent is, of course, best in all cases.
The fact that most new learners are already in practice rather than in a residency program presents challenges, but it also presents opportunities in the sense that if a robotic case is not proceeding as expected and an open procedure becomes necessary, a surgeon less experienced in robotics could return to more familiar ground.
Training programs with laboratory/simulation components would be important because of the learning curve involved, as surgeons gradually become proficient in TORS over a series of dozens of cases. 28 Programs that can provide objective data should be helpful in developing medicolegal strategies, as well.
Credentialing for TORS surgeons is left to hospitals, and the medicolegal risks of negligent credentialing for both surgeons and hospitals have been raised. 23 The claim of negligent credentialing is recognized in at least 32 states. 21 Hospitals need guidance and perhaps standardization to establish credentialing guidelines. However, with the explosion of new technology in multiple specialties, we must address the question, How can individual hospitals be expected to establish reasonable guidelines? Hospitals must walk a tightrope between welcoming new surgical technology and avoiding negligent credentialing in the eyes of the courts. National specialty associations and societies can be helpful in this regard; in fact, we believe they should take the lead.
Establishing effective training programs and guidelines should not only improve patient care and enhance surgeons’ experience and confidence, it should minimize patient dissatisfaction and the risk of litigation. Surgeons, hospitals, government and private payers, and patients all have a stake in how new technology can be Safety introduced. The development of practice guidelines, new requirements for achieving and maintaining certification, and training methods to include proctorship and simulation would be ideal.
We believe that the courts should not play a major role in establishing safety guidelines for the introduction of new technology such as robot-assisted surgery. The lengthy timeline and somewhat unscientific nature of this process does not lend itself to rigid rules and requirements, and allowances for certain imperfections must be made.
The law is not immutable, and it must be guided by thoughtful attempts to establish a process that is safe and reproducible across the nation. This would help surgeons avoid malpractice lawsuits in the first place, it would be better and less expensive for payers, and most important, it would provide safer and better care for our patients.