
Abstract
We performed a retrospective chart review to compare the presence and types of abnormal muscle tension patterns (MTPs) in patients who had been diagnosed with glottal insufficiency before and after fiberoptic injection laryngoplasty. The main cause of glottal insufficiency had been unilateral vocal fold paralysis. Our review included an analysis of the medical records and laryngeal videostroboscopic recordings of 16 patients—9 men and 7 women, aged 25 to 87 years (mean: 59). Stroboscopic frames were analyzed for the presence of one or more types of abnormal MTP. Statistical analysis was performed to determine the significance of the change in scores for type II and type III MTP before injection and 1 month after injection. Before injection laryngoplasty, 15 of the 16 patients exhibited evidence of an abnormal MTP; 10 patients had MTP II only, 2 had MTP III only, and 3 patients had both. The mean percentage of frames showing MTP (i.e., MTP score) in patients with MTP II was 66.2% before the injection and 28.9% 1 month after; the decrease was statistically significant (p = 0.001). For MTP III, the corresponding figures were 71.6 and 37.7% (p = 0.043). We conclude that injection laryngoplasty has a positive effect on reducing muscle tension in patients with glottal insufficiency.
Introduction
Muscle tension dysphonia is characterized by dysregulated laryngeal and extralaryngeal muscle activity. 1 It exists in two forms:
a primary form that belongs to the category of functional voice disorders, in which patients experience dysphonia in the absence of any organic disease affecting the vocal folds or larynx1–3; and
a secondary form, in which patients experience dysphonia in the presence of an organic vocal fold or laryngeal pathology.3,4
Reports of possible etiologies leading to increased laryngeal muscle tension are ubiquitous in the literature. Although psychological factors and vocal abuse have been traditionally implicated in abnormal laryngeal muscle tension patterns (MTPs), other possible etiologies have emerged, including the presence of laryngopharyngeal reflux and/or glottal insufficiency.2,5–7 Glottal insufficiency, which can cause the unintentional escape of air during phonation, has been attributed to several etiologies, including vocal fold paralysis or paresis, vocal fold atrophy or bowing, and vocal fold sulcus.
Despite the close relationship between glottic insufficiency and abnormal MTPs, the literature has not yet confirmed the impact that vocal fold medialization and its role as a treatment modality for glottal insufficiency has on MTPs. In a cohort study, Belafsky et al found a positive correlation between glottal insufficiency and abnormal MTPs diagnosed by videostrobolaryngoscopy. 7 They concluded that abnormal MTPs could represent a compensatory mechanism to overcome glottal insufficiency caused by vocal fold paresis, bowing, polyps, cysts, or more subtle pathologies.
Along the same line of investigation, Stepp et al studied 13 patients before and after injection laryngoplasty. 8 They found a statistically significant reduction in glottic airflow rates, strain ratings, and false vocal fold supraglottic compression after injection. On the other hand, they found no significant change in electromyographic recordings before and after injection as determined by neck surface electromyography as a measure of vocal hyperfunction. Based on these two reports, it is believed that the treatment of glottic insufficiency, when present, should improve patients’ MTPs, at least hypothetically.
The scarcity of reports in the literature on the correlation between glottal insufficiency and MTPs and the lack of consensus on the cause-and-effect relationship between the two entities inspired us to further investigate the impact of injection laryngoplasty on abnormal MTPs before and after injection. In this article, we describe.our study of this matter.
Patients and methods
Patients
We retrospectively reviewed the medical records and laryngeal videostroboscopic recordings of all patients who had been diagnosed with glottal insufficiency and who had undergone injection laryngoplasty at the American University of Beirut Medical Center from January 2014 through October 2015. Patients with vocal fold lesions such as nodules, cysts, polyps, and granulomas were excluded.
A total of 16 patients—9 men and 7 women, aged 25 to 87 years (mean: 59)—satisfied our eligibility criteria. None of these patients had undergone voice therapy before injection laryngoplasty, although this option had been discussed with each.
Study parameters
In addition to demographic data, we compiled information on the etiology of each patient's glottal insufficiency, the type of augmentation material used, and the side and site of the injections.
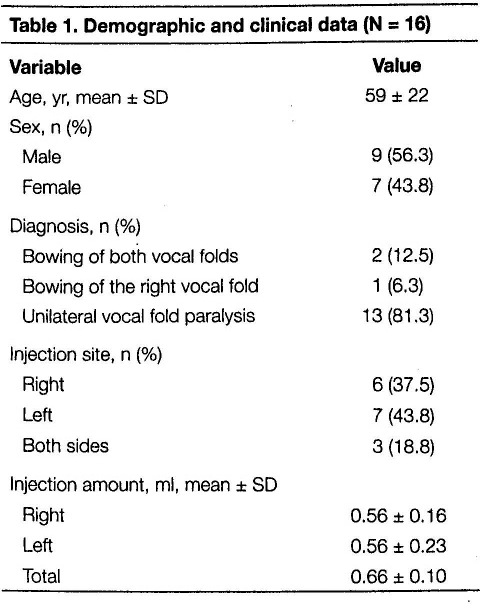
The most common etiology was unilateral vocal fold paralysis. All patients had undergone injection laryngoplasty via either the transnasal or transoral approach with a fiberoptic nasopharyngeal laryngoscope equipped with a working channel. Restylane (Q-Med AB; Uppsala, Sweden), a hyaluronic acid stabilized solution (20 mg/ml), was the augmentation material used in all patients. Six patients were injected in the right vocal fold, 7 in the left vocal fold, and 3 in both. The mean volume of injected Restylane was 0.66 ml (table 1).
Demographic and clinical data (N = 16)
Grading and calculating muscle tension patterns
The videostroboscopic images had been recorded before injection laryngoplasty and again 1 month after. The vocal task consisted of producing several iterations of the vowel /i/. The videostroboscopic frames (60 frames/sec) recorded over 2 to 3 seconds were then analyzed for the presence of one or more types of abnormal MTP. The different patterns of abnormal muscle tension were subclassified as either glottic or supraglottic, as described by Koufman and Blalock. 4 They also classified four types of abnormal MTP:
MTP I, also called a laryngeal isometric pattern, is a glottic muscle tension characterized by the presence of a gap between the vocal fold edges during phonation.
MTP II, sometimes called plica ventricularis, is a supraglottic muscle tension characterized by medial compression of the false vocal folds.
MTP III, also a supraglottic muscle tension, is characterized by an anteroposterior shortening of the distance between the epiglottic petiole and the arytenoid muscles secondary to contraction of the larynx during phonation.
MTP IV is the extreme form of supraglottic muscle tension in which there is a complete sphincter-like closure of the supraglottis during phonation.
We then computed each patient's MTP score by calculating the percentage of frames in which a single MTP was observed. The reviews of the videostroboscopic images and the calculation of the MTP scores were performed in a blinded fashion by the first author (G.Z.). The MTP score was calculated as follows:

The specific criteria used to identify and grade each abnormal MTP were as follows:
MTP I: the presence of a front-to-back gap between the vocal folds that created an open angle at the anterior commissure.
MTP II: the presence of at least a 50% medialization of the false vocal folds in relation to the distance between the middle part of the false vocal folds.
MTP III: the presence of at least one-third shortening of the anteroposterior distance between the epiglottic petiole and the arytenoid muscles.
MTP IV: the presence of a sphincter-like closure of the supraglottis with no visualization of the true vocal folds. 4
Statistical analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences software (v. 22). Baseline demographic and technical characteristics of the study population were summarized using means and standard deviations for continuous variables and percentage frequencies for categorical variables. The percentage distribution per MTP type before and after injection was also determined.
Information about patients who exhibited a reduction in abnormal MTP was described in terms of the percentage frequency (out of the total sample) and the mean change in MTP with standard deviation. The non-parametric Wilcoxon signed rank test was performed to determine the significance of changes in the percentage of MTP II and MTP III before and after injection for the study sample as a whole and among subgroups.
Statistical significance was set at p < 0.05.
Results
Before injection laryngoplasty, 15 of the 16 patients (93.8%) exhibited evidence of an abnormal MTP; 10 patients had MTP II only, 2 had MTP III only, and 3 had both. After injection laryngoplasty, all 15 patients experienced a decrease in MTP II scores (figure 1) and MTP III scores (figure 2).
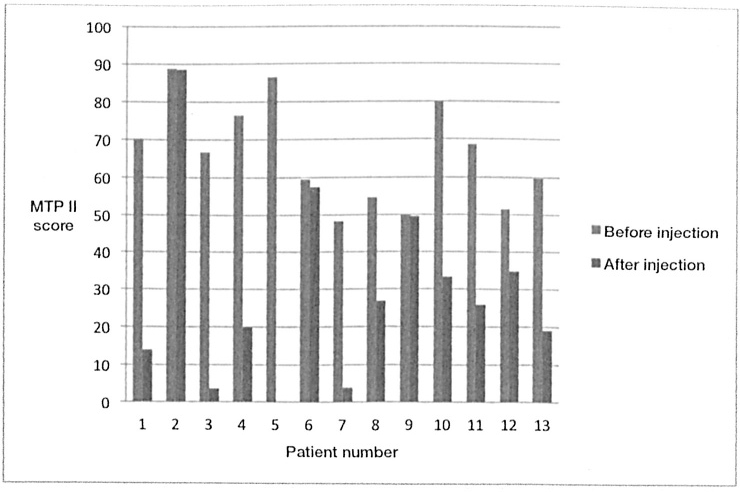
Chart depicts the distribution of MTP II scores before and after injection in the 13 patients with MTP II alone or in combination with MTP III.
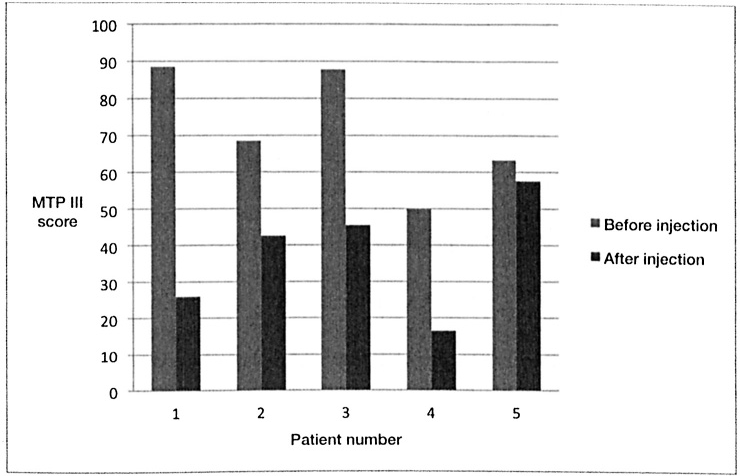
Chart depicts the distribution of MTP III scores before and after injection in the 5 patients with MTP III alone or in combination with MPT II.
The mean percentage of videostroboscopic frames showing MTP II in affected patients (i.e., the MTP score) was 66.2% before injection and 28.9% after injection—the decrease was statistically significant (p = 0.001). Likewise, the corresponding MTP III scores were 71.6 and 37.7%, which also represented a significant decrease (p = 0.043) (table 2).
Mean values of muscle tension pattern (MTP) scores before and after injection
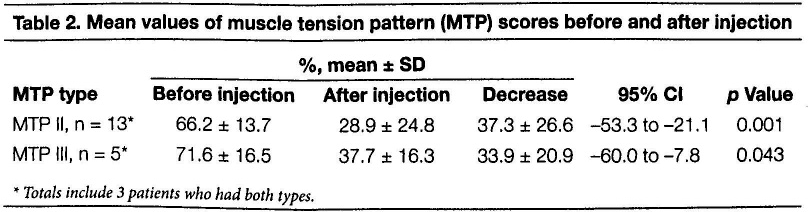
Totals include 3 patients who had both types.
We conducted a further analysis to investigate the difference in mean MTP scores among the 3 patients who had both MTP II and MTP III. This analysis revealed a decrease in MTP II score from 63.7% (±19.9) to 25.4% (±24.7) and a decrease in MTP III score from 67.3% (±19.6) to 33.5% (±21.5)—neither difference was statistically significant (p = 0.109 for both).
Discussion
First reported in 1982 by Koufman and Blalock, 9 muscle tension dysphonia characterized by altered laryngeal biomechanics has since been referred to by different terms, including functional dysphonia, hyperfunctional dysphonia, and hyperkinetic dysphonia. 2 With advances in diagnostic tools, these laryngeal bio-mechanical alterations were subsequently classified into the four types of abnormal MTP. 4 Differentiation between the various patterns and their stratification into subtypes were based primarily on findings from fiberoptic and videostroboscopic imaging. All classifications that initially listed the glottic patterns of muscle tension were later followed by listings of supraglottic patterns.4,10
There is widespread consensus in the literature that the etiology of increased laryngeal muscle tension is multifactorial, irrespective of its site of origin. 2 As reported by Belafsky et al, all possible laryngeal pathologies that cause glottal insufficiency will lead to a compensatory laryngeal behavior and subsequently an abnormal MTP. 7 Therefore, in cases where increased laryngeal muscle tension is found, it is necessary to conduct an adequate laryngeal examination with transnasal fiberoptic laryngoscopy and videostroboscopy to look for underlying laryngeal pathologies.11,12
Our study found that glottal insufficiency portends a high risk of hyperkinetic laryngeal behavior. Among the 16 patients who had been diagnosed with glottal insufficiency, 93.8% had evidence of an abnormal MTP, primarily MTP II. Furthermore, our study found that the closure of the glottal gap via injection laryngoplasty had a significant effect on decreasing laryngeal muscle tension. As such, injection laryngoplasty as a treatment for glottal insufficiency has a favorable impact on MTPs.
Treatment of the underlying glottal pathology has decreased the incidence of abnormal MTPs, thus supporting the idea that an abnormal MTP represents a compensatory hyperkinetic laryngeal behavior. Early rather than late intervention for the treatment of glottal insufficiency can be recommended for patients with a coexisting abnormal MTP.
Results similar to ours were reported by Belafsky et al, who found a preponderance of MTP II and MTP III among patients diagnosed with bowing of the vocal folds. 7 Of 100 patients who were diagnosed with glottal insufficiency, MTP II and MTP III were observed in 72 and 63 patients, respectively.
Stepp et al also reported findings similar to ours in their evaluation of 13 patients before and after injection laryngoplasty. 8 They performed acoustic, aerodynamic, and endoscopic assessments, as well as surface electromyography, before injection and 1 week after. After injection, statistically significant reductions in airflow rates and strain ratings were observed. Reductions in anteroposterior supraglottic ratings and quantitative false vocal fold compressions were also found, but they did not reach the level of statistical significance.
It is worth noting that despite our finding of a statistically significant decrease in the mean MTP score after injection in the group as a whole, there was no significant decrease in the subgroup of 3 patients who had been diagnosed with both MTP II and MTP III. We attribute this finding to the presence of multiple confounding etiologies of hyperkinetic laryngeal behavior in these patients. These etiologies can include phonotraumatic behavior, endogenous factors such as laryngopharyngeal reflux disease, psychological factors with stress exposure, and environmental factors such as allergy and noise pollution.
The multifaceted nature of an abnormal MTP and its multifactorial etiology require a comprehensive, team-based approach for diagnosis and treatment. Specifically, an efficient collaboration between laryngologists and speech therapists is essential to exploring all risk factors that might contribute to an increase in laryngeal muscular tension.
Our study has three limitations: (1) it was a retrospective investigation, (2) our sample size was limited to only 16 patients, and (3) we lacked information about confounding factors in our patients such as laryngopharyngeal reflux disease and phonatory behavior.
In conclusion, glottal insufficiency is one of the possible etiologies of abnormal MTPs, and it should be looked at when assessing a patient with increased laryngeal muscle tension. Closure of the glottal gap by injection laryngoplasty must be considered in patients diagnosed with muscle tension dysphonia secondary to glottal insufficiency. We are conducting a study to look at MTP scores in patients who undergo early vs. late injection laryngoplasty.