
Abstract
Mucoceles of the paranasal sinus can be managed endoscopically with an extremely low recurrence rate. Frontal sinus mucoceles can sometimes be prevented from closing and reforming by stenting, which to the best of our knowledge has not yet been reported in the maxillary sinus. We describe the cases of 5 patients—3 men and 2 women, aged 47 to 75 years (mean; 59.6)—with a recurrent and intractable maxillary sinus mucocele that was managed with biliary T-tube stenting. The indications for stenting included recurrent episodes of mucocele with or without a lateral location with a relatively thick bony wall. A latex rubber pediatric biliary T-tube was endoscopically inserted through a window opening into the marsupialized mucocele. The stent was removed 6 to 14 months postoperatively in 4 cases; in the other case, the stent remained adequately positioned for 35 months. None of the patients experienced signs or symptoms of recurrence. We conclude that a T-tube stent can be used successfully to maintain long-term patency in patients with a recurrent and intractable maxillary mucocele, with patency being maintained even after removal of the stent.
Introduction
Mucoceles are locally expansile paranasal sinus cysts characterized by mucous effusion. Maxillary sinus mucoceles are relatively rare, accounting for less than 10% of all paranasal sinus mucoceles described in the United States and Europe. 1 In Japan, however, maxillary sinus mucoceles are more common, usually occurring as a long-term complication of Caldwell-Luc surgery. 2
Previously, the treatment of maxillary sinus mucoceles was based on Caldwell-Luc sinusectomy, with the creation of a nasoantral window through the inferior meatus and a complete removal of the maxillary sinus lining to avoid recurrence. 3 In recent years, however, advances in endoscopic sinus techniques and instrumentation, as well as the introduction of intraoperative navigation systems, have made the endonasal approach the first choice for the treatment of maxillary sinus mucoceles.4–7
Stents have been used for more than a century to prevent stenosis, improve mucosalization, and maintain the functional patency of the paranasal sinuses, especially in the frontal sinuses. 8 However, to the best of our knowledge, there has been no report of the application of stenting for the postoperative management of recurrent and intractable maxillary sinus mucoceles.
In this article, we report a series of 5 patients with an intractable and recurrent maxillary sinus mucocele in whom long-term patency was achieved and maintained by the placement of a flexible pediatric biliary T-tube.
Patients and methods
Our study population was made up of 3 men and 2 women, aged 47 to 75 years (mean: 59.6), who underwent endoscopic sinus surgery and T-tube stenting for the treatment of a recurrent and intractable postoperative maxillary sinus mucocele at our hospital during an 18-month period. The mucoceles had been diagnosed on the basis of the surgical history and the results of computed tomography (CT). The indications for stenting included recurrent episodes of mucocele with or without a lateral location with a relatively thick bony wall.
Table. Case characteristics
Key: ESS = endoscopic sinus surgery; C-L: Caldwell-Luc surgery.
We previously described in detail the surgical technique for endoscopic marsupialization. 5 Briefly, a mucosal flap with the underlying bony wall facing the middle and/or inferior meatus is elevated from the cystic wall. When the bone is quite thick and compact, a diamond bur is required for drilling. The contents of the mucocele are evacuated with a curved maxillary sinus suction without removing the mucocele lining.
After adequate marsupialization of the mucocele is achieved, a latex rubber Deaver pediatric biliary T-tube (C.R. Bard Medical Division; Covington, Ga.) is inserted into the maxillary mucocele through the window opening. Before tube insertion, an appropriate length of T-tube is cut. In the series described here, we used a tube with an outer diameter of 15 Fr (5 mm) in 3 patients, 24 Fr (8 mm) in 1 patient, and 12 Fr (4 mm) in the remaining patient.
Our study protocol was approved by the ethics committee at the Juntendo University Faculty of Medicine. Before inclusion in this study, all patients provided written informed consent.
Results
Preoperatively, all patients complained of cheek pain and/or swelling, but none experienced nasal discharge or nasal polyps. Their previous operations for maxillary mucocele included 4 Caldwell-Luc surgeries and 3 endoscopic sinus surgeries (1 patient underwent 2 of the former and 1 of the latter). Four patients were drained through the inferior meatus; in the other, both the middle and inferior meatus were required for tube insertion (table).
Patient 1 exhibited excessive sclerosis and thickening of the bone that formed the boundary between the mucocele and the inferior meatus, which maintains the window opening of the mucocele for long-term follow-up after removal of the stent (figure 1).
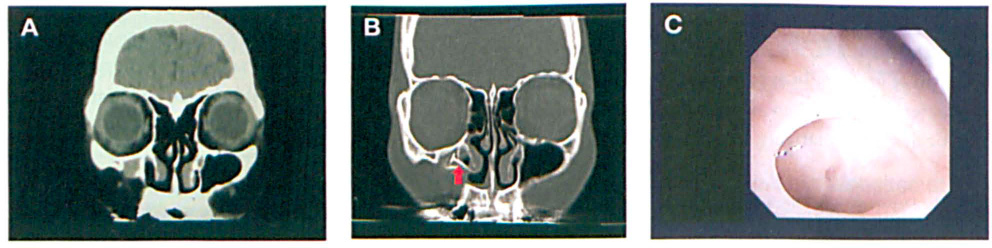
Patient 1. A: Preoperative CT shows the mucocele in the maxillary sinus. B: Postoperative image shows the T-tube (arrow) in place. C: Endoscopic view shows the window opening after the T-tube has been removed.
In patient 2, drainage was created by placing the T-tube through both the middle and inferior meatus for a laterally located maxillary mucocele (figure 2).
Patient 2.
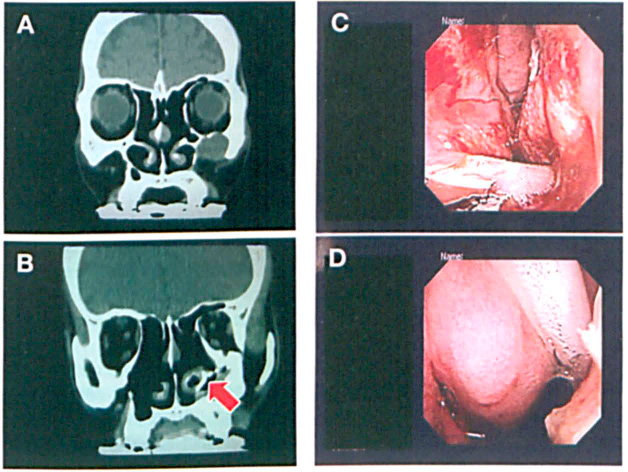
Patient 3 had had a quite intractable case of maxillary sinus mucocele, as evidenced by three previous revision surgeries. With stenting, however, the window was successfully maintained (figure 3).

Patient 3.
Postoperatively, all patients were administered an oral antibiotic, a nasal spray, and nasal irrigation. The stents were left in place for 6 to 35 months, and the total follow-up period ranged from 26 to 52 months (mean: 36). Each T-tube was removed after confirmation of proper epithelialization and aeration in the maxillary mucocele cavity by fiberendoscopy and CT.
Discussion
Even with our small number of patients, a relatively long-term follow-up confirmed that endoscopic endonasal management of recurrent and intractable postoperative maxillary mucoceles with a biliary T-tube stent should be the treatment of choice for marsupialized mucoceles.
Several conditions have been reported as risk factors for paranasal sinus mucoceles after endoscopic sinus surgery: (1) surgery during acute infection, (2) the presence of multiple mucoceles, and (3) significant extension of the mucocele outside the sinus wall. 9 Proposed contraindications to an endonasal approach to the management of maxillary mucoceles include (1) a far laterally located mucocele, (2) revision surgery with severe scar formation after a Caldwell-Luc procedure, (3) a mucocele location within the zygomatic bone, (4) the presence of a cutaneous fistula that needs to be excised, and (5) a malignancy as the cause of the mucocele. 6
The maxillary sinus mucoceles commonly seen in Japan are known as postoperative maxillary lesions that result from the obstruction of surgical ostia, especially after the Caldwell-Luc procedure.2,5 Cases that occur after a Caldwell-Luc procedure appear to involve other riskfactors for recurrence, such as recurrent episodes or a lateral location with a relatively thickened bony wall. In patients with recurrent maxillary sinus mucoceles after a Caldwell-Luc operation, excessive sclerosis and a thickened bone of the boundary between the mucocele and the nasal cavity often cause the surgically created drainage tracts to become narrow and demucosalized. With stenting, however, the patency of the drainage pathways can be maintained.
Most cases require a stent with only a small outer diameter (4 to 5 mm), which can be easily placed from the nasal meatus to the mucocele. Use of a relatively longer stent is helpful for reaching the more distant laterally or posteriorly based mucocele cavities. The stent's soft, pliable material can be manipulated for easy placement, and this can reduce the risk of insertion trauma and subsequent mucosal inflammation and reactive scar tissue formation. Furthermore, the flanges of the stents we use are custom-fit to facilitate appropriate positioning and self-retention. These stents have been used to establish long-term ventilation and have been tolerated without difficulty. 10
In conclusion, we used T-tube stenting to successfully manage long-term maxillary sinus patency in patients with recurrent and intractable maxillary mucoceles.