
Abstract
We conducted an analysis to assess the relative contribution of auditory brainstem response (ABR) testing and auditory steady-state response (ASSR) testing in providing appropriate hearing aid fitting in hearing-impaired children with difficult or unreliable behavioral audiometry. Of 150 infants and children who had been referred to us for hearing assessment as part of a neonatal hearing screening and cochlear implantation program, we identified 5 who exhibited significant discrepancies between click-ABR and ASSR testing results and difficult or unreliable behavioral audiometry. Hearing aid fitting in pediatric cochlear implant candidates for a trial period of 3 to 6 months is a common practice in many implant programs, but monitoring the progress of the amplified infants and providing appropriate hearing aid fitting can be challenging. If we accept the premise that we can assess the linguistic progress of amplified infants with an acceptable degree of certainty, the auditory behavior that we are monitoring presupposes appropriate bilateral hearing aid fitting. This may become very challenging in young children, or even in older children with difficult or unreliable behavioral audiometry results. This challenge can be addressed by using data from both ABR and ASSR testing. Fitting attempts that employ data from only ABR testing provide amplification that involves the range of spoken language but is not frequency-specific. Hearing aid fitting should also incorporate and take into account ASSR data because reliance on ABR testing alone might compromise the validity of the monitoring process. In conclusion, we believe that ASSR threshold-based bilateral hearing aid fitting is necessary to provide frequency-specific amplification of hearing and appropriate propulsion in the prelinguistic vocalizations of monitored infants.
Introduction
Early cochlear implantation in children has a positive effect on the development of the auditory pathways, as well as on postimplantation outcomes.1–3 Delays in detecting severe hearing impairment can significantly impair the development of verbal communication skills and spoken language. Thus, the implementation of universal screening of neonatal hearing is the only way to achieve very early detection of deafness and a timely referral to a cochlear implant center if need be.4,5
It is common practice to fit pediatric cochlear implant candidates who are identified by neonatal screening with bilateral hearing aids for a trial period of 3 to 6 months. If these patients do not progress linguistically, then cochlear implantation can be considered. Another rationale for fitting hearing aids in severely or even profoundly deaf infants is to provide some access to the normal auditory spectrum, taking advantage of the critical periods of neuroplasticity.6,7
The aforementioned practice in cochlear implant programs should satisfy two important prerequisites: (1) provision of appropriate hearing aid fitting and (2) monitoring the linguistic progress of the amplified infants. Both aspects can be challenging in hard-of-hearing children.
In this article, we describe our case series in which we assessed the relative contributions of auditory brainstem response (ABR) testing and auditory steady-state response (ASSR) testing in facilitating appropriate hearing aid fitting for hearing-impaired children in whom behavioral audiometry was difficult or unreliable.
Patients and methods
Over a period of 5.5 years, we assessed the hearing of 150 infants and children who had been referred to the Clinic of Pediatric Hearing Loss at Attikon University Hospital in Athens as part of a neonatal hearing screening and cochlear implantation program. The children underwent a full ENT examination, tympanometry, transient evoked otoacoustic emissions (TEOAEs) measurements, and automated ABR testing. A detailed medical and family history was also taken.
Those children whose hearing failed the initial assessment were subsequently subjected to more TEOAE measurements in addition to click-evoked ABR testing and mixed-modulation ASSR testing (90 Hz sleeping-child default mode) while they were under sedation with 4% chloral hydrate (maximum dose: 1.5 mg/kg) or, for older children, hydroxyzine HCl (10 mg/5 ml) under the guidance of a pediatrician.
Children with mild to moderate hearing loss were fitted with bilateral hearing aids and referred for speech and occupational therapy. Children with severe to profound or deteriorating hearing loss also underwent radiologic evaluation with computed tomography and magnetic resonance imaging, and they were referred for genetic testing for connexin-26 protein. They were also referred for multidisciplinary assessment in the various specialties of the cochlear implantation program. Finally, they were fitted with hearing aids for a 3- to 6-month trial.
Results
Among the 150 tested children, 5 presented with significant discrepancies between their ABR and ASSR test results (table). In these 5 children, either (1) behavioral audiometry was too difficult to be performed or (2) its results were unreliable. In these cases, hearing aid fitting was based on the information obtained by both ABR threshold testing and ASSR-predicted audiograms (figures 1 and 2).
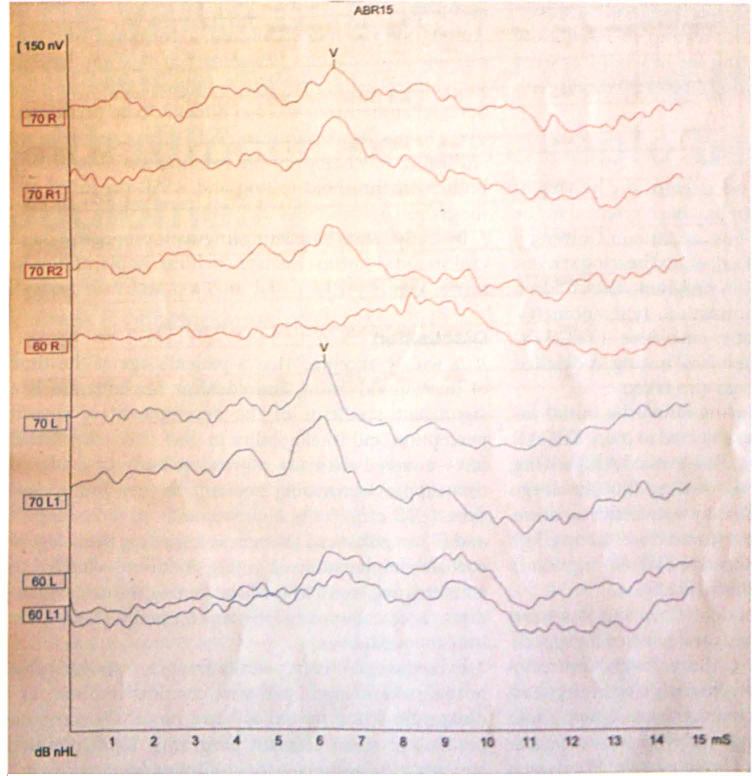
The ABR thresholds of patient 3 clearly identify wave V at 70 dB HL.
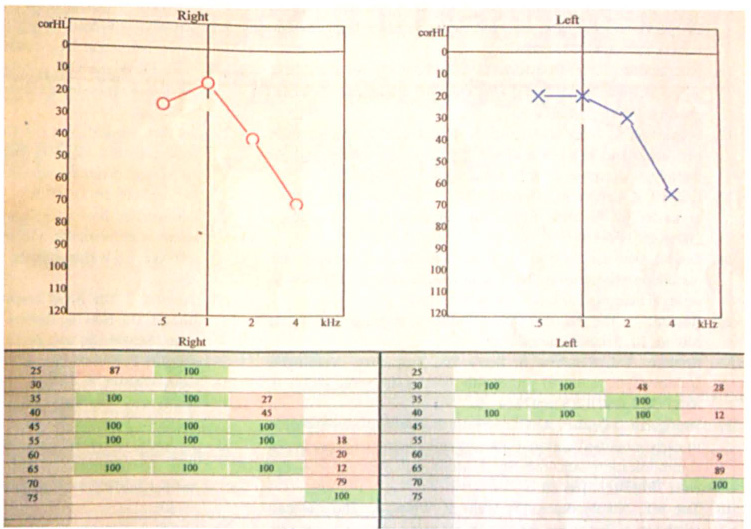
The ASSR-predicted audiogram of patient 3 clearly demonstrates the difference in ABR thresholds. (The numbers at the bottom of the figure refer to the percentage probability that the patient can hear at the corresponding dB HL.)
By study's end, the ensuing linguistic progress of these children did not necessitate cochlear implantation in any of them.
Discussion
It is widely accepted that a patient's age at the time of hearing aid fitting and cochlear implantation is a significant predictor of the development of speech perception and intelligibility in deaf children.7–11 This fact—coupled with (1) a growing body of evidence that supports providing implants to very young children (≤12 mo),1,2 (2) improvements in technology, 12 and (3) an enhanced awareness regarding the safety of cochlear implantation in young children 13 —has led to an increasing trend toward shortening the delay of auditory access to spoken language for pediatric cochlear implant candidates.
Table. General and audiologic characteristics of children presenting with significant discrepancies between ABR and ASSR test results
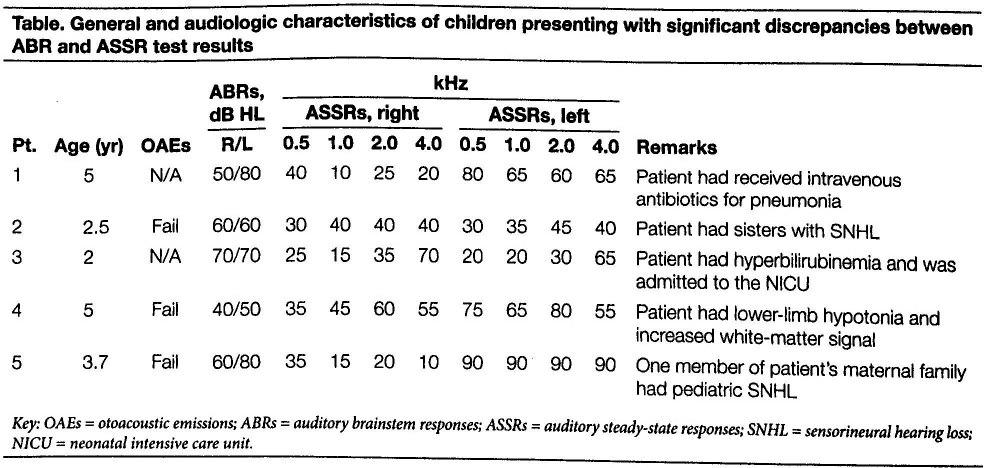
Key: OAEs = otoacoustic emissions; ABRs = auditory brainstem responses; ASSRs = auditory steady-state responses; SNHL = sensorineural hearing loss; NICU = neonatal intensive care unit.
Even though it is frequently fraught with difficulty, hearing aid fitting in pediatric cochlear implant candidates for a trial period of 3 to 6 months is common practice in many implant programs. This approach appears to be necessary for children who present with a bilateral hearing loss between 65 and 85 dB. The findings of a study by Leigh et al suggest that for severely deaf children, cochlear implantation offers a chance of about a 75% greater improvement in hearing compared with bilateral hearing aids. 14 If such a chance of improvement is probable, then cochlear implantation should be considered for hearing-impaired children who fail to demonstrate linguistic progress during a hearing aid trial. If linguistic progress during the trial is demonstrated, cochlear implantation can be postponed or cancelled.
In view of the challenges encountered in a hearing aid trial, we should note that objective outcomes of hearing amplification in infancy are usually considered to be “soft,” as they are in the vast majority subjective and often indirect (i.e., assessing parental views),15,16 or may even easily reach a ceiling effect in some cases. 17
The development of communication skills in hearing-impaired infants can be assessed by examining their preverbal communication skills. 18 Preverbal behaviors are natural precursors of language development in all children, irrespective of their hearing status. These behaviors include appropriate eye contact, conversation-al-style turn-taking, autonomy, and auditory awareness of the sound of speech. 18 They form the normal pattern of language development, which begins in early infancy.
The Tait video analysis is a fine example of a methodology for assessing preverbal communication in infants.18,19 It can also be used to monitor the development of vocal and auditory preverbal skills in very young deaf children who have been using acoustic hearing aids.
If we accept the premise that we can assess the linguistic progress of amplified infants with an acceptable degree of reliability, the auditory behavior that we are monitoring presupposes appropriate bilateral hearing aid fitting. Fitting might become very challenging in young children, and even in older children whose behavioral audiometry is unreliable due to limited cooperation or other disabilities. However, even this challenge could be addressed by using data from ABR and/or ASSR testing.
Considering the vague and non-frequency-specific information obtained from click ABRs, it is obvious that fitting attempts based on these data may not address the hearing needs of amplified children; even worse, they might lead to unpleasant or even harmful hearing. Therefore, click ABR testing should not be the only method of monitoring children's preverbal progress, especially in cases where behavioral audiometry is unreliable.
Even though tone-burst-evoked ABRs have been used to estimate the configuration of hearing loss in children, technical issues along with the amount of time needed to record electrophysiologic thresholds seem to limit their applicability. 20 Hence, hearing aid fitting should take into account ASSR data to ascertain the validity of the fitting and monitoring processes.
Our case series involves a subpopulation of hearing-impaired children with significant discrepancies between the results of their ABR and ASSR tests. These discrepancies might prove to be challenging for appropriate hearing aid fitting when reliable behavioral audiometry is not available. For example, in our patient 3, the 70-dB ABR threshold waveform referred to the 4.0-kHz frequency only (figures 1 and 2). The remaining frequencies appeared to be normal or borderline. Fitting this child with a uniform amplification of 55 to 60 dB in all frequencies likely would have resulted in intolerance to the use of the hearing aids, which would understandably hinder the child's auditory and vocal progress. If this were to pose a problem for a 2-year-old such as our patient 3, the issue could be even more serious in infants due to the limitations mentioned above, and it could compromise the validity of the monitoring process.
The idea that ASSRs might be a more accurate predictor of behavioral thresholds than are ABRs in certain patients with steeply sloping hearing loss has been previously supported by other investigators.21,22 ASSR thresholds can be used to predict the configuration of pure-tone audiometry,23,24 which would contribute to an appropriate bilateral hearing aid fitting in hard-of-hearing infants. However, the potential difference between pure-tone and ASSR thresholds in the hearing-impaired population—which usually does not exceed 7 dB (±5), depending on the frequency25,26—should also be considered, both during the fitting process and when determining cochlear implant candidacy.
In conclusion, appropriate management of hearing-impaired children should ensure that they will receive the maximum amount of auditory information during the critical periods for spoken language development and thereby achieve age-appropriate spoken language skills to the closest extent possible. Moreover, we must ensure that a reliable monitoring process is established for the group of children who are in a hearing aid trial before cochlear implantation. To achieve this, especially in children with difficult or unreliable behavioral audiometry, ASSR threshold-based bilateral hearing aid fitting is necessary to provide frequency-specific amplification of hearing and appropriate propulsion in the prelinguistic vocalizations of monitored infants.