
Abstract
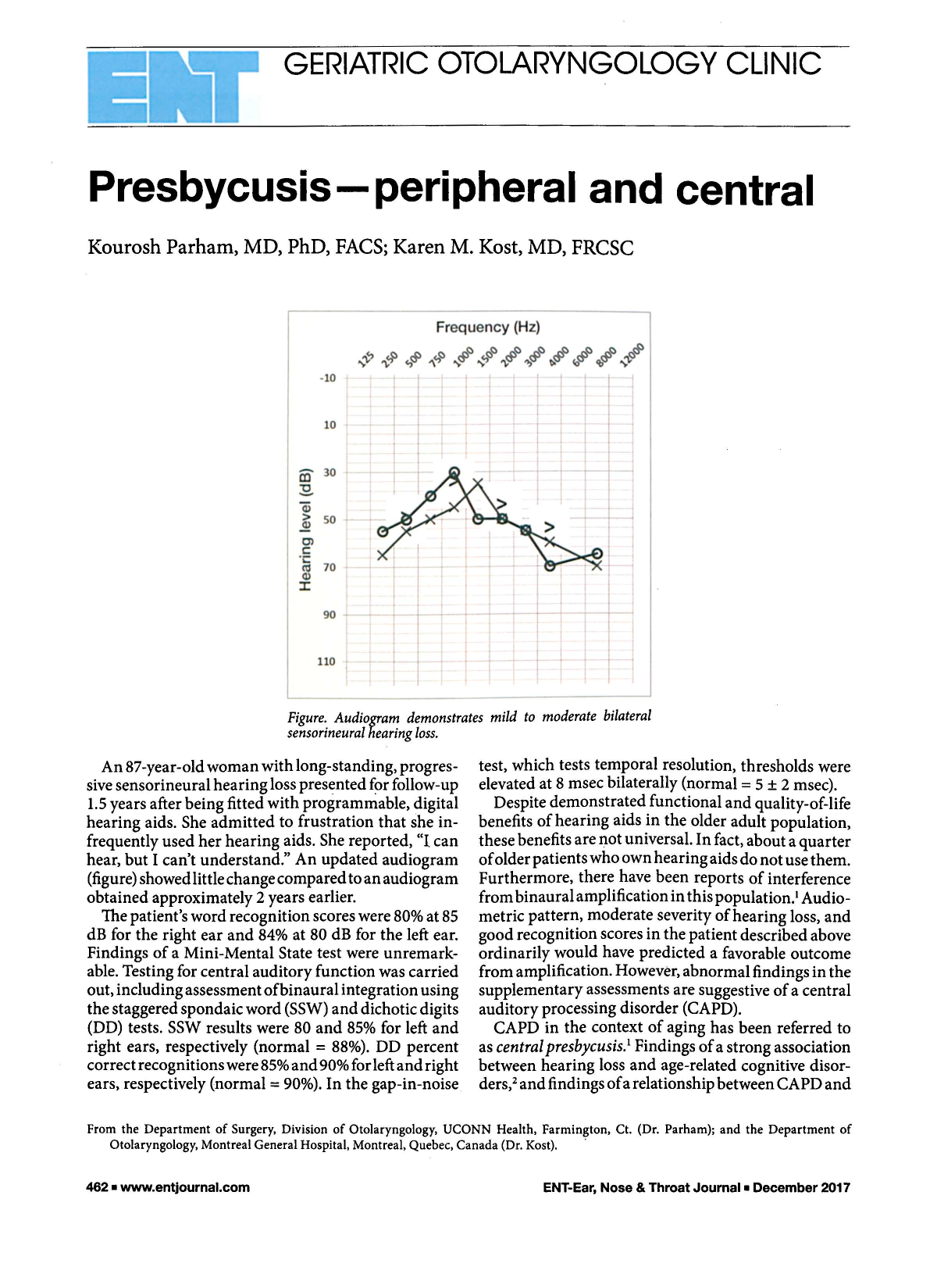
Figure. Audiogram demonstrates mild to moderate bilateral sensorineural hearing loss.
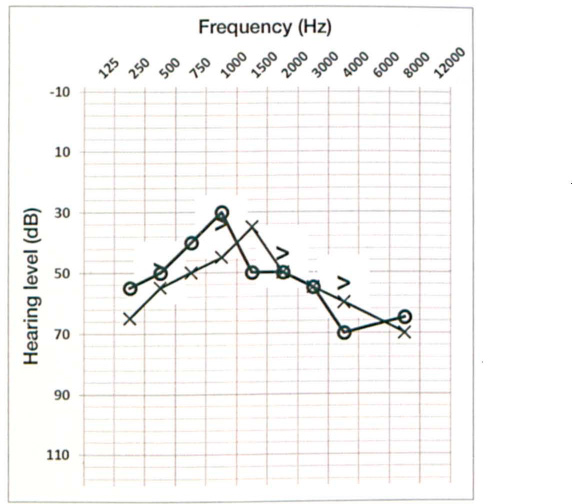
An 87-year-old woman with long-standing, progressive sensorineural hearing loss presented for follow-up 1.5 years after being fitted with programmable, digital hearing aids. She admitted to frustration that she infrequently used her hearing aids. She reported, “I can hear, but I can't understand.” An updated audiogram (figure) showed little change compared to an audiogram obtained approximately 2 years earlier.
The patient's word recognition scores were 80% at 85 dB for the right ear and 84% at 80 dB for the left ear. Findings of a Mini-Mental State test were unremarkable. Testing for central auditory function was carried out, including assessment of binaural integration using the staggered spondaic word (SSW) and dichotic digits (DD) tests. SSW results were 80 and 85% for left and right ears, respectively (normal = 88%). DD percent correct recognitions were 85% and 90% for left and right ears, respectively (normal = 90%). In the gap-in-noise test, which tests temporal resolution, thresholds were elevated at 8 msec bilaterally (normal = 5 ± 2 msec).
Despite demonstrated functional and quality-of-life benefits of hearing aids in the older adult population, these benefits are not universal. In fact, about a quarter of older patients who own hearing aids do not use them. Furthermore, there have been reports of interference from binaural amplification in this population. 1 Audio-metric pattern, moderate severity of hearing loss, and good recognition scores in the patient described above ordinarily would have predicted a favorable outcome from amplification. However, abnormal findings in the supplementary assessments are suggestive of a central auditory processing disorder (CAPD).
CAPD in the context of aging has been referred to as central presbycusis. 1 Findings of a strong association between hearing loss and age-related cognitive disorders, 2 and findings of a relationship between CAPD and age-related cognitive disorders including Alzheimer disease,3-5 have highlighted the importance of assessing CAPD in the workup of presbycusis. These associations strongly suggest central presbycusis's being a progressive, neurodegenerative disease. 6 Therefore, rehabilitation strategies in older adults with CAPD findings need to be more comprehensive than fitting hearing aids, which are designed to compensate for peripheral deficits. 1
Rehabilitation may be facilitated through introduction of communication programs that include auditory training, speechreading, and auditory-visual training coupled with improvements in communication strategies, conversational fluency, assertiveness, stress management, and personal adjustment. 7 Emerging research investigating benefits of auditory training in patients with CAPD, including older adults, demonstrates efficacy of programs that include, for example, dichotic interaural intensity difference training that can be administered using customized stimuli through an audiometer. 8
Unfortunately, older adults rarely undergo CAPD testing, and relatively few audiologists offer either individual or group communication programs. This shortcoming is driven by poor understanding of the mechanisms underlying central presbycusis, limited research into outcomes of rehabilitation strategies, and a lack of economic incentives for additional services and research. The burgeoning geriatric population, particularly in those >85 years of age, makes it imperative to address these gaps in the care of older patients.