
Abstract

The most common malignancy of the nasopharynx is nasopharyngeal carcinoma. However, nasopharyngeal papillary adenocarcinoma is a rare primary tumor of this location. This tumor shows a remarkable papillary architecture, arising from the surface epithelium and in general showing indolent biologic behavior. There are no known etiologic agents, lacking any Epstein-Barr virus or human papillomavirus association.
Patients with this tumor tend to be young (mean: 4th decade) at presentation, without a sex difference. Nasal obstruction is the most common symptom, although otitis media or postnasal drip may be seen with the tumor involving the posterior and lateral nasopharyngeal walls. The tumor is slowly growing, showing only a local recurrence potential and lacking metastatic documentation.
Nasopharyngeal papillary adenocarcinoma may appear grossly as an exophytic, nodular, or polypoid mass, sometimes gritty if psammoma bodies are present. The tumor is composed of a complex, arborizing, and interwoven papillary architecture, usually showing hyalinized fibrovascular cores (figure 1). The tumors invade into the underlying stroma. The papillae are lined by a single layer of cuboidal to columnar cells that have abundant cleared to eosinophilic cytoplasm (figure 2). The nuclei are usually optically cleared, showing grooves, folds, and irregular nuclear membranes, reminiscent of papillary thyroid carcinoma.
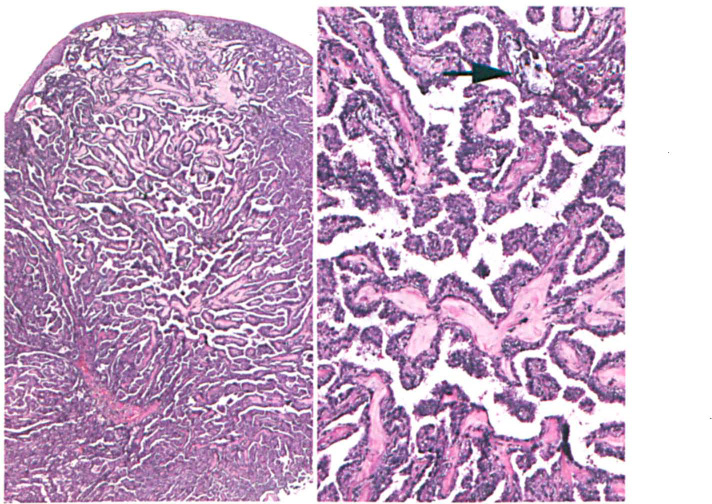
Left: The surface epithelium overlies an arborizing, complex papillary neoplastic proliferation. Right: There are cuboidal to columnar cells lining the papillary structures; the fibrovascular cores are heavily collagenized. Psammoma body calcifications are noted (arrow).
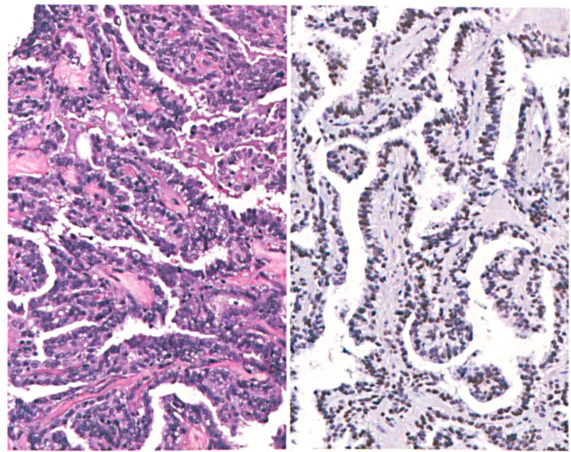
Left: There is little pleomorphism, although nuclear contour irregularities, grooves, and folds are seen. Right: A strong and diffuse nuclear TTF1 immunoreactivity is seen.
In general, mitoses and necrosis are absent. The tumor cells react with CK7, CK5/6, and EMA, and will also show strong TTF1 immunoreactivity (figure 2). Obviously, the latter finding supports the thyroid-like low-grade nasopharyngeal papillary adenocarcinoma nomenclature sometimes applied. However, the tumors do not express thyroglobulin. The differential diagnosis includes metastatic papillarythyroid carcinoma, sinonasal papilloma, and selected minor salivary gland carcinomas (such as polymorphous adenocarcinoma).