
Abstract
Bone-anchored hearing aid (BAHA) implants deliver sound using vibrations passed through an osseointegrated implant. Drawbacks with a skin-penetrating implant include the need for daily skin care and skin-related complications. To address these issues, manufacturers developed magnet-based conduction implants (MBCIs) that use magnetic coupling to transcutaneously attach a sound processor with a magnet external to the skin to an osseointegrated implant with a magnet beneath the skin.
Magnetic coupling must to be strong enough to steady the device and deliver energy for sound conduction while not being so strong as to injure the interposed skin and soft tissue. Skin complications are rarely reported with MBCIs in the literature.1-7 However, we present a case of pressure-induced skin necrosis in an MCBI patient who had adequate soft tissue and skin but had undergone many prior local surgeries. We also describe the method of soft-tissue repair.
A 27-year-old African American woman with Treacher Collins syndrome and bilateral mixed hearing loss had previously undergone left-sided microtia repair, as well as left ear canal atresia repair, with subsequent restenosis and persistent hearing loss. She had had a left percutaneous, bone-anchored hearing aid placed 4 years before visiting the authors. She reported excellent hearing outcomes but had repeated skin overgrowth and infections requiring three different procedures to revise the skin, despite using the longest compatible abutment (9 mm).
Four months after her last skin revision, the skin hypertrophy had worsened and she presented to the authors, desiring a new magnet-based system. After reviewing the options of continued local care or replacement with a new percutaneous implant and longer abutment at an adjacent site, she chose to proceed with the MBCI.
Under general anesthesia, the prior abutment was removed along with an elliptical cuff of the hypertrophic skin. A new implant site superior to the former site was chosen to ensure that all skin covering the new magnet would be uninvolved from the prior wound site. The skin was measured to be 7 mm thick. A BAHA Attract (Cochlear Americas; Denver) implant and magnet were placed, and the skin flap slightly thinned to 6 mm (confirmed with a soft-tissue gauge).
After 4.5 weeks, the skin over the magnet appeared well healed, and the processor was loaded with a No. 4 magnet. Two weeks later, the patient returned with dry, fully necrotic crust under the magnet site (figure 1). Although she understood the instructions to limit early use, the patient admitted that a personal emergency had compelled her to wear the processor throughout each day to better hear, and to ignore early irritation and drainage from the site. By the time she could contact the physician, the site was no longer draining or painful, so the processor was still being worn over the necrotic crust.

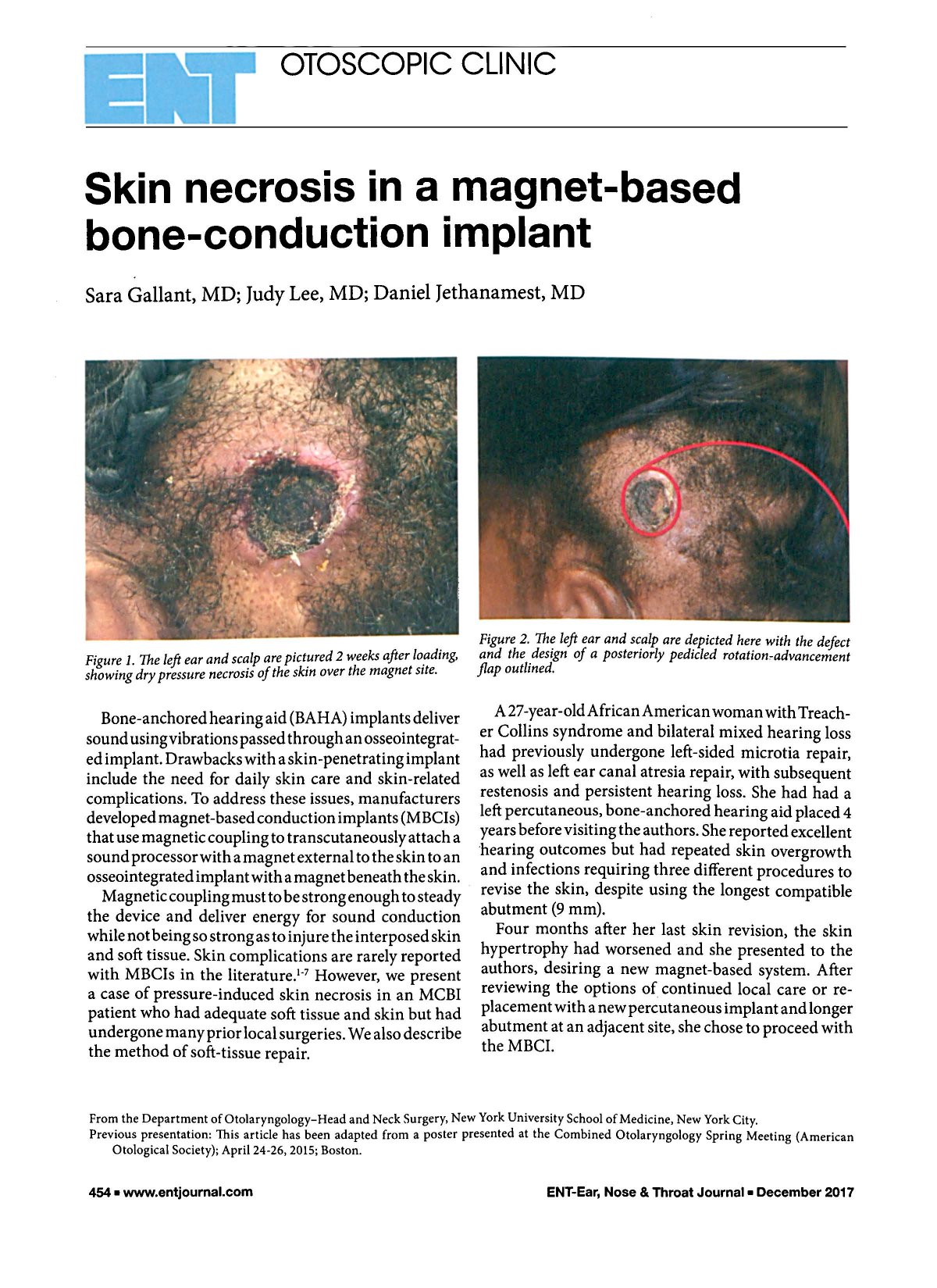
The left ear and scalp are pictured 2 weeks after loading, showing dry pressure necrosis of the skin over the magnet site.
After a review of options, the patient's preference was to repair tissue and return to a percutaneous system. She underwent wound exploration, removal of the magnet, and placement of a cover screw. Given the left temporal scalp defect from skin necrosis, a rotation-advancement flap pedicled posteriorly from the occipital vessels was used (figure 2). The flap was widely undermined to allow closure of the defect with reduced wound tension. There was complete closure of the defect at postoperative follow-up, and delayed placement of a subsequent abutment was planned (figure 3). The patient used a Baha Softband hearing device (Cochlear Americas; Centennial, Colo.) while the scalp flap was observed for adequate healing.

The left ear and scalp are depicted here with the defect and the design of a posteriorly pedicled rotation-advancement flap outlined.

The well-healed wound site is shown 2 weeks after rotation-advancement flap repair.
Two months after the flap repair, the patient underwent placement of a longer hydroxyapatite-coated abutment under local anesthesia. She has since been using the processor without skin complications for more than a year.
Multiple factors likely contributed to the pressure necrosis seen in this case. The pressure-bearing skin over an MCBI may be affected by prior local surgeries. Patients with complicated wound sites or multiple surgeries should be counseled to carefully monitor their skin as they have reduced sensation. Conservative initial magnet strengths should be used in these patients.
Although we cannot determine whether the skin changes would have been reversible with early cessation of use, as is reported in other MBCI series,5,6 the prolonged early duration of use against recommendations likely played a large role in our patient's skin necrosis. The importance of discontinuing device use if any abnormality is detected should be reiterated to patients, and they should be followed closely. A local scalp rotation-advancement flap is an effective technique to rapidly address this complication with good cosmetic outcomes.