
Abstract
Ossifying fibromyxoid tumors are rare soft-tissue neoplasms, usually with an indolent course. However, atypical/ malignant variants have been described, showing either local recurrence after complete excision or metastasis to the lungs, mediastinum, adrenals, or soft tissue. We report the case of an ossifying fibromyxoid tumor of the left ankle that metastasized to the lung and thyroid gland 12 years after the initial diagnosis and surgical treatment. To our knowledge, this is the first reported case of this neoplasm metastasizing to the thyroid gland.
Introduction
Ossifying fibromyxoid tumors of soft parts (OFMTs) are rare soft-tissue neoplasms. 1 They are usually small, painless, and well circumscribed, and commonly arise in the subcutis or muscle of the extremities; less often, they arise from the trunk or head and neck region. 1
Microscopically, these tumors are partially lobulated, containing small, round cells with vesicular nuclei and minute nucleoli, arranged in cords within a fibromyxoid matrix. 2 A peripheral rim of collagen with metaplastic bone is commonly present, but cases lacking bone formation have been described. 3
Although OFMTs are often benign, reports have described atypical variants that exhibit local recurrence after complete local excision, as well as distant metastasis to the lung, mediastinum, adrenals, or soft tissue.4–6 We report the case of a variant of malignant OFMT that originated in the leg and metastasized to the lung and thyroid. A single case of OFMT originating in the prethyroidal soft tissue with direct extension into the thyroid was described by Lax et al 7 in 1995, but to our knowledge, ours is the first reported case of metastatic OFMT to the thyroid.
Case report
A 55-year old woman presented with a mass in her left ankle. Biopsy of the lesion revealed an intermediate-grade sarcoma, possibly a variant of malignant OFMT. The patient underwent a left below-knee amputation, and pathology of the resection specimen confirmed this diagnosis. The margins of resection were negative for tumor. The patient had no postoperative adjuvant therapy, but she was closely followed for 12 years with no evidence of recurrence.
Twelve years after her initial OFMT diagnosis, the patient presented to an emergency department with left chest and upper shoulder pain. Initial evaluation, including a multi-gated acquisition scan, revealed no cardiac ischemia. However, chest x-ray showed a large mass in the lower lobe of the left lung with an associated pleural effusion. Biopsy of this lesion revealed a spindle-cell neoplasm, most consistent with metastatic disease from her original sarcoma.
Further workup with computed tomography of the chest, abdomen, and pelvis confirmed the presence of a lung mass measuring 11.5 × 7.2 cm. Three indistinct, smaller nodules were also found in the lung. Incidentally, a 3.6-cm nodule was seen in the thyroid isthmus. Subsequent positron-emission tomography showed a standard uptake value (SUV) in the larger, lower left lung mass of 3.5 and an SUV of 3.4 in the thyroid nodule. The smaller, indistinct masses in the lung were inactive. A bone scan was also performed and was unremarkable.
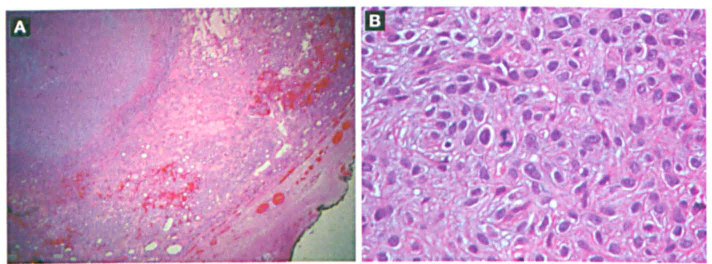
Figure. A: Metastatic focus of OFMT is seen in the thyroid parenchyma (hematoxylin and eosin; original magnification × 25). B: Higher-power view shows atypical mitotic figures, with moderately sized epithelioid cells in a fibromyxoid background (hematoxylin and eosin; original magnification x400).
The patient underwent left lower-lobe resection; pathology on a section of the lingula revealed a low-grade fibromyxoid sarcoma consistent with metastatic disease. Further workup of the thyroid nodule with ultrasound demonstrated multiple masses, with a dominant mass measuring 2.5 cm in the right lobe of the thyroid. Ultrasound-guided fine-needle aspiration of this mass was interpreted as a follicular neoplasm, and a decision was made to perform right hemithyroidectomy and isthmusectomy.
Pathology of the thyroid revealed that the larger, more prominent mass seen by ultrasound was consistent with an adenomatous nodule. However, a distinct, 0.6-cm focus showing moderately sized epithelioid cells within a fibromyxoid background was also present. Histologically, this lesion was similar to that seen in the ankle and lung, consistent with metastatic disease.
The initial left ankle lesion was composed of areas containing bland and uniform ovoid to spindled cells with hyperchromatic nuclei distributed in a vaguely corded pattern, scattered in a collagenous matrix. Very few mitoses were present in these areas. However, other areas had much higher cellularity, with nuclear pleomorphism and scattered multinucleated giant cells. Osseous and cartilaginous metaplasia was also focally present. Given these characteristics, the lesion was classified as an intermediate-grade sarcoma, consistent with an atypical/malignant variant of OFMT.
The thyroid tumor nodule was described as a white, well-circumscribed, slightly firm nodule measuring 0.6 cm in diameter. Microscopically, this nodule was composed of moderately sized epithelioid cells with indistinct cell borders, fibrillary cytoplasm, and round to irregular nuclei with clumped chromatin within a fibromyxoid background (figure). Focally, single cell necrosis and increased mitotic activity (up to 22 mitoses per 10 high-power fields) were seen. Overall, the lung and the thyroid lesions shared similar histopathologic features, consistent with metastatic disease from the same ankle primary.
Discussion
Primary mesenchymal tumors of the thyroid are uncommon. Metastasis to the thyroid gland is a relatively infrequent finding in clinical practice, occurring in the setting of widely metastatic melanoma and carcinoma of the breast, kidney, or lung. 8 Sarcomas metastatic to the thyroid are extremely rare and occur almost exclusively in cases of malignant fibrous histiocytoma (undifferentiated pleomorphic sarcoma), leiomyosarcoma, and liposarcoma.8–10 To our knowledge, this is the first report of OFMT metastasizing to the thyroid gland.
OFMT was first described by Enzinger et al in 1989 as a neoplasm that has a largely benign histologic appearance and clinical course, occurs in patients ranging in age from 14 to 83 years, and has a slight male preponderance.1,11 Multiple reports have described OFMT variants with either atypical or frankly malignant histology that behave in a more aggressive manner, either with local recurrence after complete excision or with distant metastasis to various sites.
In the follow-up of 51 cases, Folpe et al found metastatic disease in 8 cases (mean follow-up time of 54 months); additional case reports have described 2 cases of OFMT metastatic to the lungs.5,6,12 Furthermore, reports have described aggressive behavior in histologically bland-appearing tumors with metastasis and eventual death of the patient.11,13 However, because of the rarity of this tumor, its behavior and the sites to which it metastasizes are not well characterized.
Immunohistochemical staining patterns of OFMT lesions vary greatly. Approximately 70% of OFMTs are positive for S-100 protein and vimentin, but this percentage decreases considerably in atypical and malignant variants of the disease. 2 Positivity for keratins, smooth muscle actin, collagen II, desmin, leu-7, and glial fibrillary acidic protein have also been described.2,6
Our patient had a known history of OFMT that was labeled as an atypical/malignant variant because of the high cellularity and nuclear pleomorphism it displayed. The pulmonary nodule appeared more than 12 years after the initial diagnosis. Since the lungs are the most common site for metastasis of these tumors, clinical suspicion for metastatic disease was high. Although the lung lesion displayed mild cellularity without pleomorphism, mitotic figures, and necrosis, the overall appearance was more consistent with metastasis rather than a separate new primary.
In conclusion, we present the case of an atypical/malignant variant of OFMT that metastasized to the lung and thyroid gland more than 12 years after the initial diagnosis. Given the largely unknown clinical behavior of and prognosis for these tumors, close follow-up of patients with OFMT is recommended.