
Abstract
Ten rhinoplasty operations performed using postauricular fascia for the purpose of augmenting the radix and dorsum of the nose were analyzed retrospectively. All the operations were performed over a 1-year period, between 2005 and 2006. The fascia of the postauricular area has been used as a source of pliable soft-tissue grafts in primary and revision rhinoplasty. It may be easily accessed using a single sulcus incision that also enables harvesting of ear cartilage grafts. Deficiency in the radix is an overlooked abnormality seen in many patients undergoing primary as well as revision rhinoplasty after aggressive hump removal. Recent trends in rhinoplasty have been to avoid the overly reduced nasal skeleton and to create a more balanced nasal surgery result. This article presents the use of the postauricular fascia as a radix graft that has been found to be simple to carry out, reliable, and long lasting. In addition, the fascia graft is useful in the camouflage of various nasal deformities in the dorsum and sidewalls. The average patient follow-up for the study was 24 months.
Introduction
Postauricular fascia previously has been identified as a potential source of grafts for various reconstructive procedures.1–11 It has been used in the reconstruction of the eye socket in combination with hydroxyapatite spheres. 1 Others have designed various vascularized flaps from postauricular fascia for ocular, auricular, and otologic surgery.2–5 When the fascia has been used as a free graft, the results have been reliable. 1
Vascularized tissue transfers require extensive knowledge of the anatomy and meticulous technique in order to preserve the vascular structures involved.7–11 However, while variations occur with regard to the muscular contributions, the fascial layer has been found to be consistent in providing a durable graft.1,12
Many aesthetic rhinoplasty techniques primarily involve a reduction operation. 13 While this concept is valid for large noses, it cannot be universally applied. Modern rhinoplasty places an emphasis on appropriate diagnosis and correction of nasal deformities. Augmentation rhinoplasty techniques are used to bring the nasal structure into balance and to avoid aggressive reduction that can produce inferior aesthetic and functional results. Many types of material have been used for augmentation, including autologous tissue.14–16 Autologous tissue has been found to be the most reliable, particularly for revision rhinoplasty. 17
In this article, postauricular fascia is described as an autologous donor tissue that was found to produce a durable and pliable graft for rhinoplasty augmentation. Use of the postauricular fascia graft can produce predictable results in rhinoplasty patients requiring soft-tissue augmentation.
Patients and Methods
We retrospectively analyzed the charts of 10 rhinoplasty patients in whom surgery was performed over a 1-year period using postauricular fascia to augment the dorsum of the nose. Factors examined in this study included maintenance of augmentation, prolonged edema, infection, extrusion, wound complications, and premature resorption of the soft-tissue restoration.
Operative Technique
Preoperative antibiotics and corticosteroids are given, and the donor site is injected with 1% lidocaine and 1:100,000 epinephrine. The donor site is approached before the nasal operation commences. An incision is made in the auricular sulcus (figure 1). A subcutaneous dissection of the postauricular skin is performed, and the postauricular fascia is exposed as the skin flap is retracted (figure 2). Depending on the requirements at the recipient site, a graft of various sizes can be obtained. The fascia is incised near the auricle sulcus, and a subfascial dissection is performed.
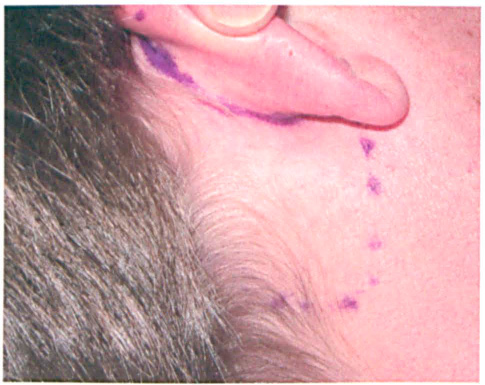
Photo shows the preoperative markings for the auricular sulcus incision and dissection area.
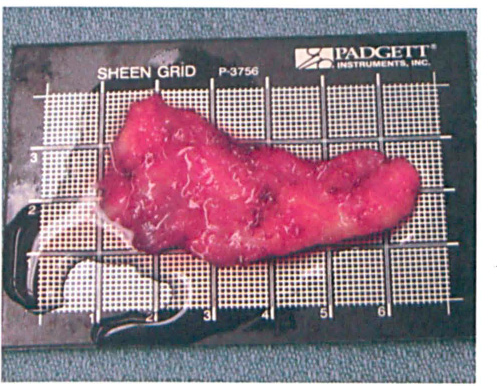
In this photo, the exposed fascia component is seen before folding and suturing.
The superior, inferior, and posterior dimensions of the flap are outlined during dissection, and the flap is harvested. In some cases, the fascia must be cleaned of attached muscle bundles. Auricular cartilage grafts should be harvested after the fascia is harvested. A small drain is left in the donor site, and the incision is closed with absorbable suture. This technique can be used for open or endonasal surgery.
During rhinoplasty, the areas of augmentation are prepared to establish the smoothest contour possible for graft placement. The postauricular fascia graft is particularly useful for radix augmentation, but it may also be used to camouflage irregularities on the dorsum and nasal sidewalls. Cartilage grafts can also be wrapped in postauricular fascia. Before graft placement, the recipient site is irrigated with antibiotic solution.
Radix Augmentation
For radix augmentation, the graft is prepared using a previously described technique. 18 The graft is folded to fit the size of the recipient area and sutured together with a4-0 plain gut suture (figure 3). The needle is left attached to the suture. An overcorrection of 25% is planned. 18 With the nasal skin retracted, the tip of the suture needle is brought out through the skin high in the radix while the graft is guided into the radix. A Steri-Strip is used to hold the suture and graft in place.
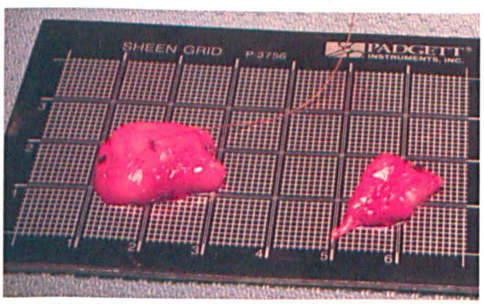
The folded fascia graft is constructed with absorbable suture.
Postauricular fascia is thicker than temporal fascia but can be folded to wrap diced cartilage grafts. Small dorsal deformities can be camouflaged using the fascia alone. Fascia grafts used in the dorsum and sidewalls are held with suture.
Results
A total of 8 primary and 2 revision rhinoplasty procedures were performed over a 12-month period. In 6 patients, the fascia was used solely to augment the radix. Another 4 patients had combinations of grafts placed in the radix and dorsum. One patient had fascia placed in the nasal sidewalls. The largest graft obtained measured 7 × 7 cm, with an average size of 4 cm2. The measured thickness of the graft was variable, less than 1 mm at the margins and up to 2.4 mm centrally. The donor site drain was typically removed by the second postoperative day.
In all cases studied, satisfaction with the results of nose surgery was high (figure 4). The results of radix augmentation with fascia were noted to be excellent with an average 24-month follow up (figure 5).

Patient is seen before (left photos) and 3 years after (right photos) fascia graft radix augmentation.

Patient is seen before (left photos) and 2 years after (right photos) nasal surgery with a postauricular fascia graft.
Two patients experienced complications. One patient developed a hematoma in the donor site that required drainage. A second patient, in which fascia was used for radix augmentation, required revision tip rhinoplasty for tip asymmetry 1 year after surgery. Infection, displacement, extrusion, and resorption were not seen in this series. Corticosteroid injections to the supratip area for prolonged swelling were required in 2 patients.
Discussion
Postauricular fascia is an underutilized soft-tissue structure that can consistently deliver a pliable graft for augmentation in rhinoplasty. The postauricular fascia is created by the fascial contributions of 7 muscles located in the postauricular region. 12 This muscle complex has several variations. However, the fascial component is consistently thick enough to provide an adequate graft.3,12 Dissection of the fascia is straightforward, and the surgeon typically does not encounter major blood vessels or important facial nerve branches behind the ear.1,12 A sizeable graft, on average 4 cm2, may be obtained.
The incision in the auricular sulcus is hidden and highly cosmetic. Access to the fascia is obtained by extending the incision inferiorly and superiorly along the sulcus, without the risk of alopecia, which may be seen with the harvest of temporal fascia. 19 Some surgeons make separate incisions to obtain auricular cartilage and temporal fascia, but in using the sulcus, access to both fascia and cartilage with a single incision is possible.
Recent publications demonstrate the advantage of using a single postauricular incision to obtain small composite, full-thickness skin-fascia-fat grafts for nasal tip reconstruction. 6 Another report describes a similar incision used to obtain a chondrocutaneous graft from the postauricular area for nasal reconstruction. 20
While alloplastic materials are an alternative to autologous tissue in rhinoplasty, human fascia from the patient is more likely to be accepted and less likely to become infected, resorbed, or extruded. 21 Fascia also is more likely to allow revascularization than alloplastic materials. 21 Evidence suggests that diced cartilage grafts wrapped in fascia are more likely to survive completely, be metabolically active, and resist absorption when compared to cartilage wrapped in alloplastic material. 22
Infections, premature resorption, and extrusions were not seen in this study population. Nasal tip swelling and development of a fluid collection at the donor site in 1 patient required treatment. Revision tip rhinoplasty was required for another patient who received a radix fascia graft.
Placement of fascia in the radix has been previously described and is a relatively simple procedure. 18 Soft-tissue defects in the dorsum, nasal sidewalls, or in revision rhinoplasty may be more challenging. To avoid mishaps at the recipient site, we take great care in preparing the recipient bed before graft implantation. Any uneven bone spurs or irregularities are treated to create the smoothest surface possible. For greater accuracy in placement, an attempt is made to hold all grafts in place with sutures.
Deficiency in the radix is an overlooked abnormality seen in patients undergoing primary as well as revision rhinoplasty after aggressive hump removal. 23 Recent trends in rhinoplasty have been to avoid the overly reduced nasal skeleton and to create a more balanced nasal surgery result. A key component is the preoperative identification of the deep nasofrontal angle. While surgeons previously reduced the nasal dorsum to the level of the low radix, emphasis on a natural profile has focused attention on deficiency in the radix region.
Radix cartilage grafts serve as alternatives to fascia grafts and historically have been used by surgeons for longer periods. 15 Use of cartilage grafts requires a high level of experience to prevent the grafts from becoming palpable or appearing displaced after the surgical swelling goes down. 18
This article describes a simple alternative technique for treatment of the low radix that requires little experience with augmentation rhinoplasty. The harvest of the fascia is simple and the tissue is readily available, especially in revision cases. The overwhelming concern with soft-tissue grafts has traditionally been premature resorption. Meticulous sterile technique, use of antibiotic irrigation, delicate tissue handling, and overcorrection of the low radix by 25% are steps that can increase the reliability of these nasal grafts.
With an average follow-up of 24 months postsurgically, this study supports the concept that postauricular fascia provides long-lasting augmentation in rhinoplasty and can provide a natural aesthetic result.