
Abstract
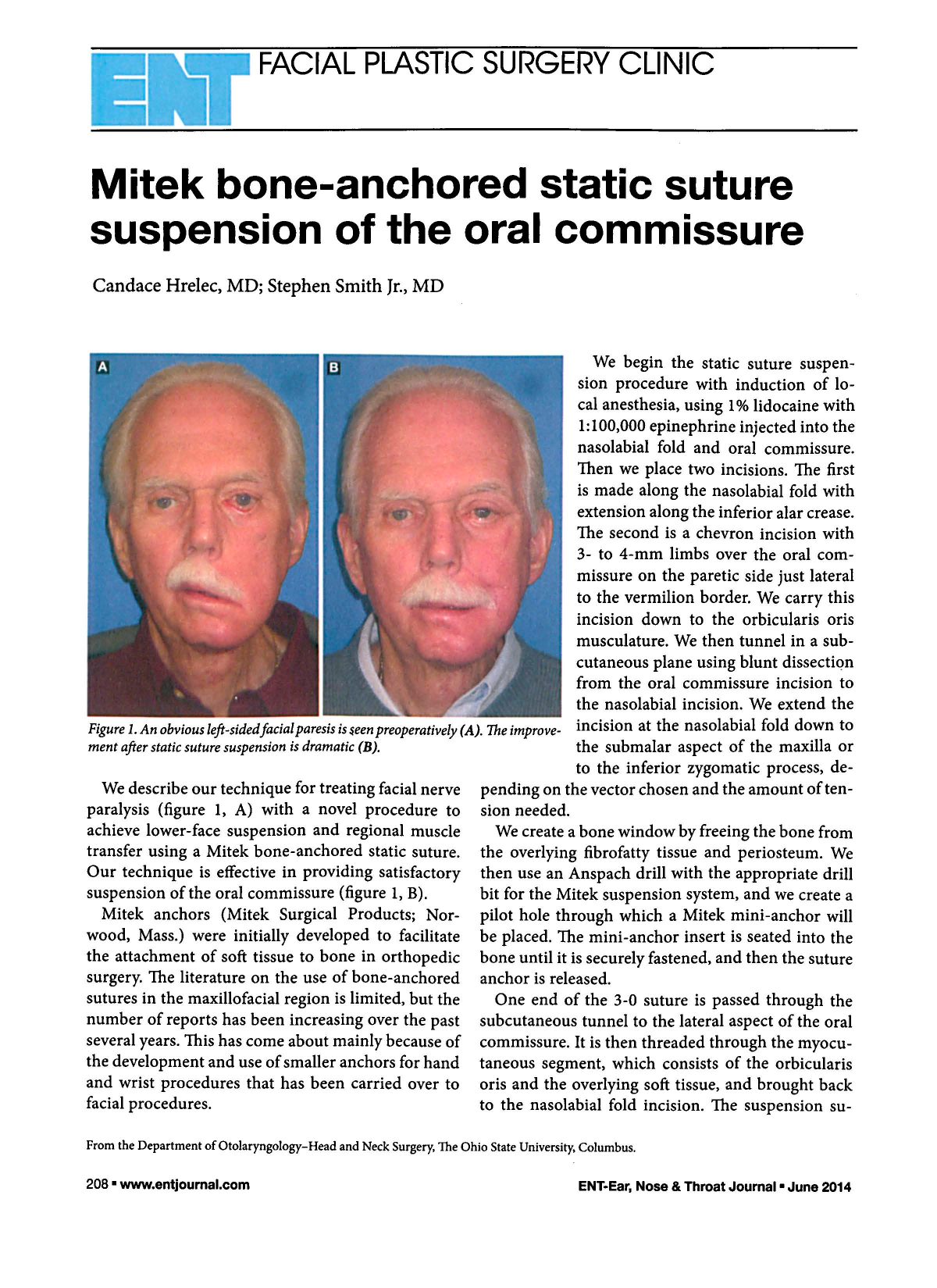
We describe our technique for treating facial nerve paralysis (figure 1, A) with a novel procedure to achieve lower-face suspension and regional muscle transfer using a Mitek bone-anchored static suture. Our technique is effective in providing satisfactory suspension of the oral commissure (figure 1, B).
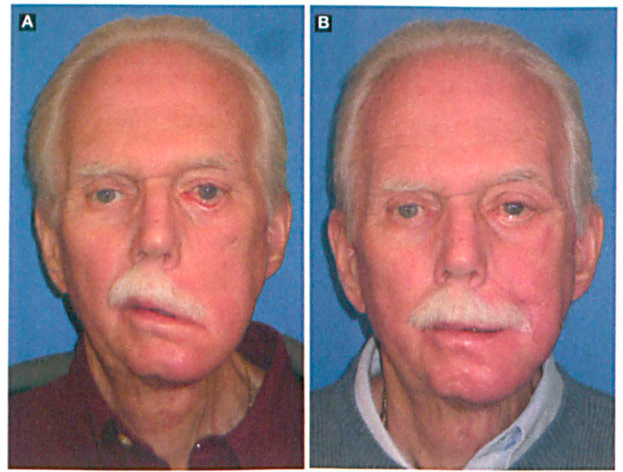
An obvious left-sided facial paresis is seen preoperatively (A). The improvement after static suture suspension is dramatic (B).
Mitek anchors (Mitek Surgical Products; Norwood, Mass.) were initially developed to facilitate the attachment of soft tissue to bone in orthopedic surgery. The literature on the use of bone-anchored sutures in the maxillofacial region is limited, but the number of reports has been increasing over the past several years. This has come about mainly because of the development and use of smaller anchors for hand and wrist procedures that has been carried over to facial procedures.
We begin the static suture suspension procedure with induction of local anesthesia, using 1% lidocaine with 1:100,000 epinephrine injected into the nasolabial fold and oral commissure. Then we place two incisions. The first is made along the nasolabial fold with extension along the inferior alar crease. The second is a chevron incision with 3- to 4-mm limbs over the oral commissure on the paretic side just lateral to the vermilion border. We carry this incision down to the orbicularis oris musculature. We then tunnel in a subcutaneous plane using blunt dissection from the oral commissure incision to the nasolabial incision. We extend the incision at the nasolabial fold down to the submalar aspect of the maxilla or to the inferior zygomatic process, depending on the vector chosen and the amount of tension needed.
We create a bone window by freeing the bone from the overlying fibrofatty tissue and periosteum. We then use an Anspach drill with the appropriate drill bit for the Mitek suspension system, and we create a pilot hole through which a Mitek mini-anchor will be placed. The mini-anchor insert is seated into the bone until it is securely fastened, and then the suture anchor is released.
One end of the 3-0 suture is passed through the subcutaneous tunnel to the lateral aspect of the oral commissure. It is then threaded through the myocutaneous segment, which consists of the orbicularis oris and the overlying soft tissue, and brought back to the nasolabial fold incision. The suspension suture is then used to create a weave within the facial modiolus and the soft tissues deep to the nasolabial fold. The suture is tied down and secured in the expected superior and lateral trajectory and distance with a slight overcorrection in order to elevate the oral commissure and nasolabial fold. The redundant skin of the upper cutaneous lip is then advanced and resected, and a layered closure is performed with buried 5–0 Maxon and running 6–0 Prolene sutures for skin closure (figure 2).

The redundant skin of the nasolabial fold is excised, and a new nasolabial fold is created in a natural position.
Static facial suspension plays an important role in long-standing facial nerve paralysis, and techniques continue to evolve. Although other procedures are less morbid and invasive than our dynamic facial technique, they also have their complications and limitations. For example, autologous facial sling grafts, including the fascia lata graft, result in morbidity at the donor site, require multiple incisions, and are prone to recurrence of facial ptosis with laxity of the graft. Recurrence of facial ptosis secondary to sling laxity is also the most common complication of allograft slings, as satisfactory cosmetic results last only about 6 months with AlloDerm.
Postoperative infection has also been observed, as has graft extrusion, which is a particular problem with Gore-Tex slings in patients who undergo postoperative irradiation. Newer techniques such as the multivector suture technique have disadvantages that include suture failure from breakage.1–3
Newer applications for the bone-anchored suture system include nasal valve suspension for correction of nasal valve obstruction. Friedman et al found that more than 90% of patients enrolled in their study exhibited an improvement in their nasal airway. 4 The bone anchor suture system has also been used in medial canthoplasty with extension over to lateral canthoplasty in recent years with promising results.5,6
In a recent study, Yu et al concluded that the Mitek mini-anchor system is a simple and effective means of improving oral-nasal competence and oral commissure and upper lip symmetry; although long-term results were not available, oral commissure elevation persisted at 6 months. 7 We believe the advancement and removal of redundant upper lip tissue that is a part of our technique may prove to be a useful adjunct.
The advantages of the bone-anchored suture technique over the more traditional methods include (1) relatively small incisions that can be camouflaged in the nasolabial crease and vermilion border, (2) minimal dissection, (3) burial of the anchor under the bone surface, (4) the simplicity of the procedure with suture, (5) ease of suture removal, and (6) the overall mechanical strength of the system, which allows for suspension of a large tissue mass.8,9