
Abstract
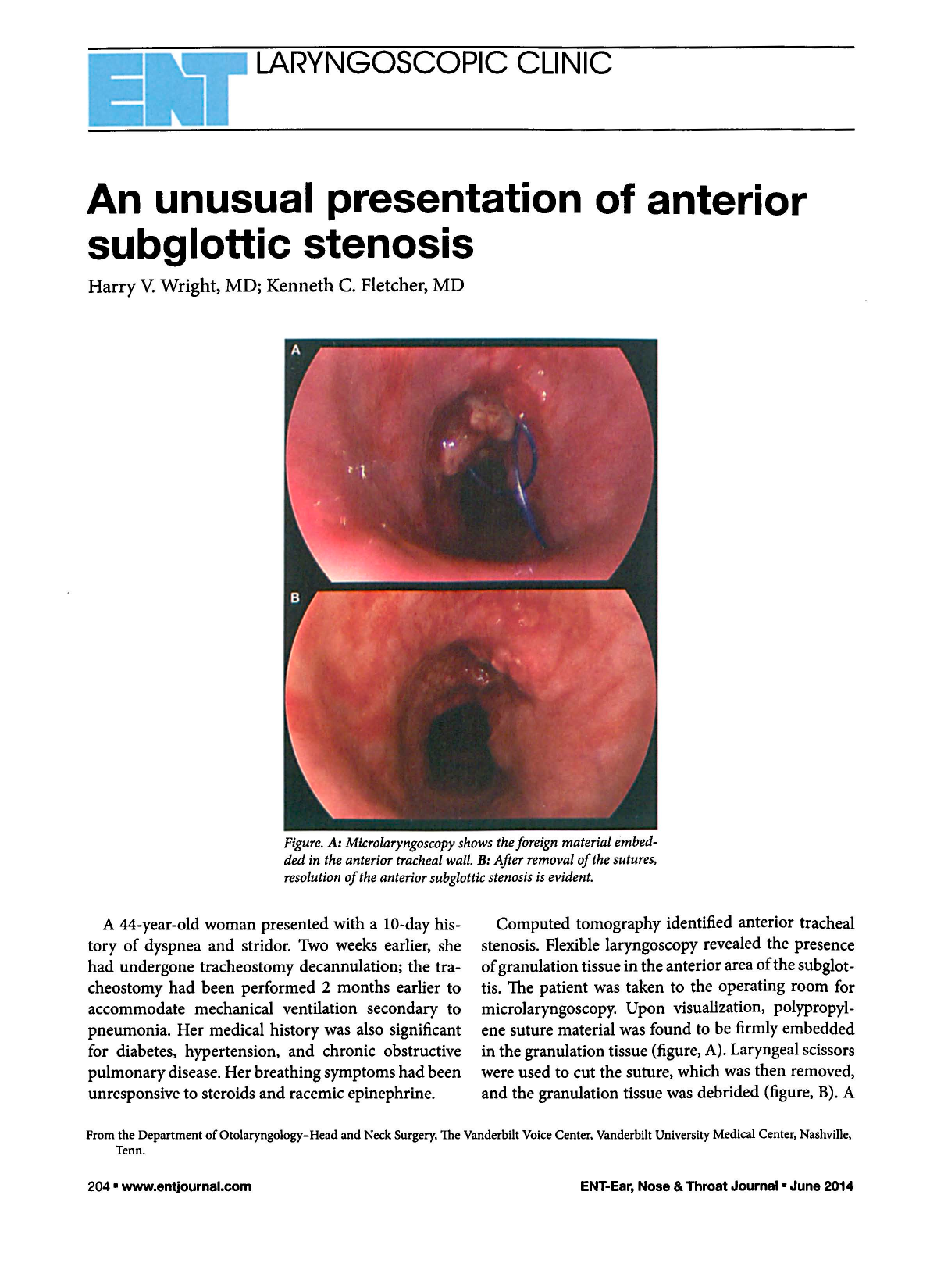
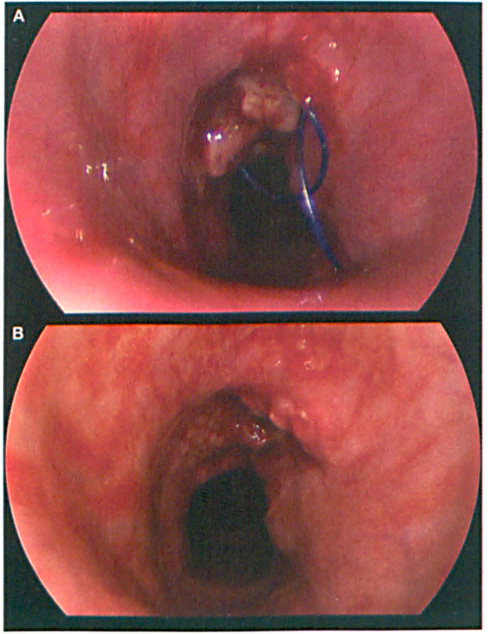
Figure. A: Microlaryngoscopy shows the foreign material embedded in the anterior tracheal wall. B: After removal of the sutures, resolution of the anterior subglottic stenosis is evident.
A 44-year-old woman presented with a 10-day history of dyspnea and stridor. Two weeks earlier, she had undergone tracheostomy decannulation; the tracheostomy had been performed 2 months earlier to accommodate mechanical ventilation secondary to pneumonia. Her medical history was also significant for diabetes, hypertension, and chronic obstructive pulmonary disease. Her breathing symptoms had been unresponsive to steroids and racemic epinephrine.
Computed tomography identified anterior tracheal stenosis. Flexible laryngoscopy revealed the presence of granulation tissue in the anterior area of the subglottis. The patient was taken to the operating room for microlaryngoscopy. Upon visualization, polypropylene suture material was found to be firmly embedded in the granulation tissue (figure, A). Laryngeal scissors were used to cut the suture, which was then removed, and the granulation tissue was debrided (figure, B). A dynamic collapse of the anterior tracheal wall was noted at the area of the previous tracheostoma. Balloon catheter dilation was performed at the level of the prolapse, and the airway was widened significantly. After the patient awoke from the anesthesia, she exhibited complete resolution of her dyspnea and stridor.
The larynx and trachea are semirigid cylindrical structures in which wound healing processes tend to stenose the lumen. Subglottic stenosis is a well-known late complication of tracheostomy, occurring in approximately 1 to 8% of reported cases.1,2 Symptoms usually develop 2 to 12 weeks following decannulation. 3 The etiology of subglottic stenosis following tracheostomy includes ischemia, devascularization, and granulation tissue. 4 In this case the exuberant granulation tissue and obstruction likely occurred as a result of the foreign body.
Our review of the notes from our patient's previous surgery, which had been performed at another institution, revealed that a Prolene stay suture had been placed during her tracheostomy. Placement of a stay suture during surgical tracheostomy is advocated for improving control of the airway intraoperatively and for the emergency management of inadvertent decannulation. 5 Stay sutures are typically removed at the time of decannulation. In this case, it seems likely that the failure to remove the sutures led to their subsequent migration through the tracheal wall, and the resultant foreign-body reaction led to the development of the subglottic stenosis.
This case illustrates the importance of removing nonresorbable stay sutures at the time of decannulation. As an additional safeguard, many practitioners place absorbable stay sutures. Finally, acquired subglottic stenosis should be suspected in any patient with unexplained dyspnea weeks to months following decannulation.