
Abstract
At their earliest stage, pathologic lesions of the laryngeal epithelium are macroscopically invisible. Ideally, these lesions should be detected before their clinical manifestations appear so that prompt management can be initiated. However, most diagnostic modalities are unable to detect early premalignant lesions. We conducted a retrospective study of the use of contact endoscopy in analyzing the vocal fold mucosal epithelium in adults who had been operated on at our hospital under general anesthesia for various nonlaryngeal diseases. After we identified 71 such patients who were smokers, we chose an almost equal number of nonsmokers (n = 70) for comparison purposes. In all, our study population was made up of 141 patients—51 men and 90 women, aged 21 to 78 years (mean: 52). All patients had normal findings on preoperative laryngeal endoscopy. Our goal was to determine if the routine use of this diagnostic modality is justified in selected cases. Contact endoscopy identified dysplastic vocal fold lesions in 4 patients and chronic laryngitis in 3; all 7 of these patients were smokers. Since early laryngeal lesions are not macroscopically evident, early detection of these changes by other means is associated with a better prognosis and easier management. Our study demonstrates that the use of contact endoscopy during general anesthesia as a standard diagnostic method in long-time cigarette smokers is fully justified.
Introduction
Even the mildest abnormality of the vocal folds can lead to hoarseness. Ideally, changes in the vocal fold mucosa will be detected early on, before they manifest clinically. One diagnostic modality that is useful in this regard is contact endoscopy. This noninvasive method provides an insight into the microscopic picture of laryngeal mucosa epithelium. With this simple and noninvasive method, cells are analyzed in vivo, thus avoiding the possibility of cell damage and distortion.
Contact endoscopy was first described by Hamou et al in 1984 in a gynecologic diagnosis. 1 In the 1990s, Andrea et al reported the use of contact endoscopy in examining the vocal folds 2 and the nasal mucosa. 3 Arens et al 4 confirmed the efficacy of contact endoscopy in examining the larynx, and Cikojević et al 5 demonstrated that it was superior to frozen-section histopathology in diagnosing laryngeal pathology. These and other studies6–9 have shown that contact endoscopy is a reliable method in the diagnosis of malignant and premalignant diseases.
In this article, we describe our study of contact endoscopy in examining the epithelium of the vocal fold mucosa in smokers and nonsmokers who were free of clinical symptoms of laryngeal disease.
Patients and Methods
For this retrospective study, we studied the use of contact endoscopy to analyze the mucosal epithelium of the vocal folds of 71 smokers who were operated on at our hospital under general anesthesia for the treatment of various nonlaryngeal diseases. For comparison purposes, we chose an almost equal number of nonsmokers (n = 70) who had undergone the same type of procedures. In all, our study population was made up of 141 patients—51 men and 90 women, aged 21 to 78 years (mean: 52). Indications for surgery included thyroid disease, nasal septal deviation, nasal polyposis, cervical cysts, and other conditions. All patients had normal findings on preoperative laryngeal endoscopy.
Upon induction of endotracheal anesthesia, the vocal fold mucosa was stained with 1% methylene blue. After 1 minute, a contact endoscope was placed against the vocal fold and moved along it from the anterior commissure toward the posterior aspect. The examination was captured on video. This was done on both vocal folds. A pathologist later analyzed the video images. A biopsy for histopathology was not routinely performed during the procedure; however, a biopsy was subsequently recommended for those patients who were found to have a pathologic lesion.
Findings on contact endoscopy were classified into four categories: normal mucosa, chronic laryngitis, dysplasia, and squamous cell carcinoma:
Normal mucosa
The stratified squamous epithelial cells are homogeneously distributed. The nuclei are small, pyknotic, and dark blue, and the cytoplasm is large and light blue (figure 1).
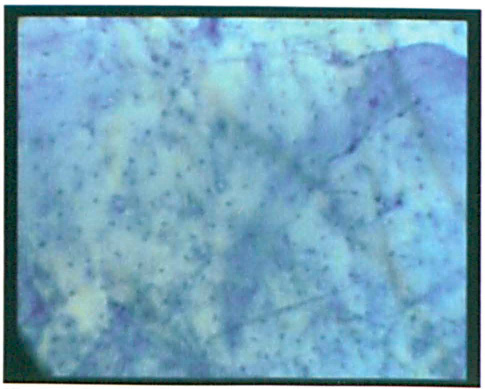
Contact Endoscopy Shows Normal Vocal Fold Epithelium (Original Magnification x 60).
Chronic laryngitis
Cells are homogeneously distributed. The nuclei are slightly enlarged, and they have rounded edges. There might be slight hyperchromatism, but chromatin is uniformly and finely granulated and free of major chromatin abnormalities (figure 2).
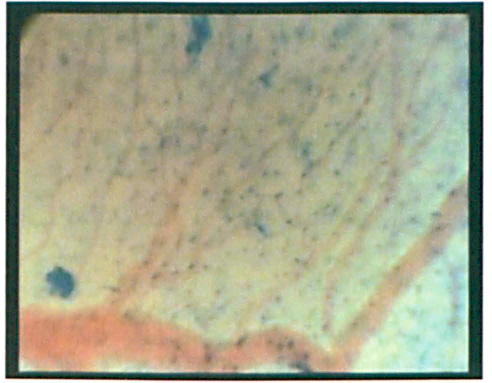
This view shows chronic laryngitis with regular microvasculature of the vocal fold (original magnification x60).
Dysplasia
The cell population is heterogeneous. The nuclei are enlarged, variedly shaped, and hyper-chromatic. The nucleus-to-cytoplasm ratio is weighted in favor of the nucleus. There is an increase in the number of mitoses, and dyskaryosis, anisokaryosis, and dyschromatosis are present (figure 3).
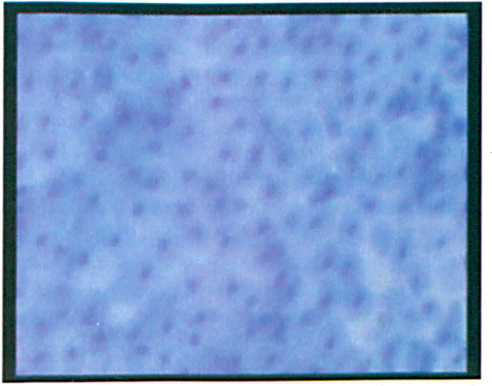
This View Shows Dysplasia (Original Magnification x150).
Squamous Cell Carcinoma
There is a pronounced heterogeneity of the cell population. Nuclear hyperchromatism and an irregular chromatin distribution are seen, and there is an increase in the size and number of irregularly shaped nuclei. The nucleus-to-cytoplasm ratio is tilted in favor of the nucleus.
Our study was approved by our hospital's Ethics Committee, and written informed consent was obtained from all patients.
Results
Contact endoscopy detected abnormal findings in 7 of the 71 smokers (9.9%) and in none of the nonsmokers. Four smokers had a dysplastic vocal fold lesion (1 grade I lesion and 3 grade II lesions) and 3 had chronic laryngitis.
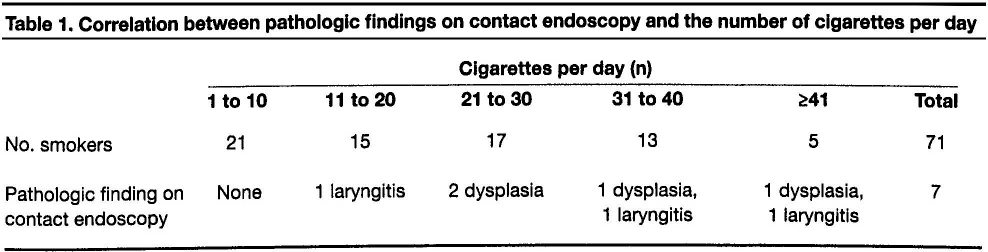
A higher incidence of premalignant pathology was associated with a greater number of cigarettes per day. No pathologic lesions were observed in 21 patients who smoked 10 or fewer cigarettes per day (table 1).
Correlation between Pathologic Findings on Contact Endoscopy and the Number of Cigarettes Per Day
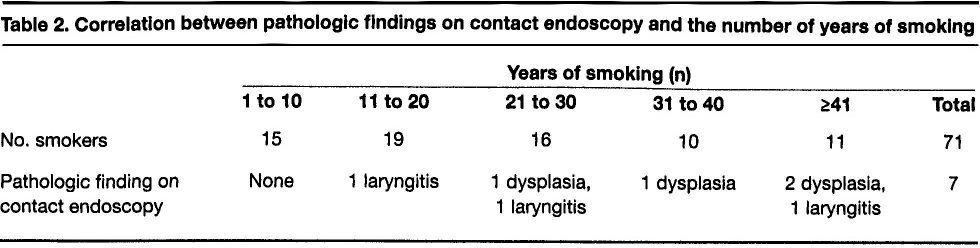
The severity of the pathologic vocal fold findings was directly proportional to the length of time the patient had been a smoker. All 15 patients who had smoked for 10 years or less were free of pathologic lesions. The incidence of lesions was substantially higher in patients who had smoked for 20 years or more (table 2).
Correlation between Pathologic Findings on Contact Endoscopy and the Number of Years of Smoking
Discussion
Approximately 98% of all patients with laryngeal carcinoma are long-time smokers.10–12 Therefore, we would expect to find a higher prevalence of early premalignant laryngeal lesions in this population. In our study, contact endoscopy demonstrated early pathologic findings in 7 of the 71 smokers (9.9%) and in none of the 70 nonsmokers.
Contact endoscopy is the only diagnostic method that enables precise in vivo microlocalization of early vocal fold lesions. As a result, macroscopically invisible changes can be identified, and sampling of the target site can be performed. It is true that exfoliative cytology can also identify macroscopically occult lesions, but this method requires sampling of the entire vocal fold surface, and therefore the precise location of the pathologically altered cells is difficult to determine. 13
Healthy and pathologically unaltered mucosa can be visualized on autofluorescence endoscopy. Healthy mucosa appears as a greenish area, while altered mucosa is reddish or purple. 4 However, this method does not provide a microscopic image of the lesion, and inflammation frequently yields false-positive results.
Contact endoscopy, on the other hand, provides insight into the mucosal microvascularization; enhanced and regular microvascularization indicates an inflammatory process (figure 2), and pathologic microvascularization points to a malignancy. The growth of a tumor is accompanied by development of its own microvascularization, which is irregular and easily discernible on contact endoscopy.
The findings of our study were in concordance with others in that the development of a laryngeal lesion was more common in smokers than nonsmokers and that it was directly correlated with the number of cigarettes per day and the number of years a patient had been smoking.10–12 Others have shown that the prevalence of both precancerous lesions and benign lesions (e.g., polyps, cysts, etc.) is also greater in cigarette smokers. 10 Early detection of macroscopically invisible laryngeal lesions is associated with a better prognosis and easier management. It is noteworthy that some laryngeal lesions disappear when the irritating factor (e.g., smoking) is eliminated.14,15
Our study demonstrates that the use of contact endoscopy as a standard diagnostic method in long-time cigarette smokers during procedures performed with general anesthesia is fully justified. This noninvasive method should also be performed in smokers with voice alterations because it provides a microscopic insight into the nature of pathologic lesions of the vocal fold mucosa epithelium.