
Abstract
We used the IB-question Glasgow Benefit Inventory (GBI) to conduct a retrospective assessment of quality of life following nasal valve surgery. We telephoned 53 patients who had undergone open rhinoplasty for the treatment of nasal valve collapse over a 2-year period. A total of 39 patients—24 men and 15 women, aged 20 to 50 years (mean: 38)—agreed to participate and answer the questions. Follow-up ranged from 3 to 12 months (mean: 8). The spectrum of possible GBI scores ranges from −100 (maximum negative outcome) to 0 (no change) to +100 (maximum benefit); in our group, the median total score was +56 (interquartile range: +32 to +90.5) and the overall total score was +58. The three subscale components of the GBI—general benefit, physical benefit, and social benefit—were analyzed individually; the respective median scores were +46 (+21 to +71), +67 (+25 to +91.5), and +50 (+17 to + 100), and the respective overall scores were +60, +59, and +50. Based on these findings, we conclude that nasal valve surgery significantly improves quality of life.
Introduction
The nasal valve area is the narrowest portion of the nasal passage and hence a common site of nasal airway obstruction. Because nasal valve collapse can be easily overlooked, it is often not properly managed. 1
The surgical treatment of disorders of the nasal valve requires a thorough knowledge of nasal anatomy, physiology, and pathology.
Anatomy
The external valve consists of the ala, the skin and fibrofatty tissue of the vestibule, the nasal sill, and the contour of the medial crus of the lower lateral cartilage. 2 The external valve has a tendency to collapse in the setting of a high rate of airflow, even in normal individuals. It can be weakened by the effects of aging, surgery, and trauma. 3
The internal nasal valve is thought of in two aspects: the internal valve area and the internal nasal valve angle. These are distinct terms that should not be confused:
The internal nasal valve area is a space bounded medially by the septum and superiorly and laterally by the caudal margin of the upper lateral cartilages and its fibroadipose attachments to the piriform aperture and the anterior end of the inferior turbinate. Inferiorly, it is made up of the floor of the piriform aperture. 1
The internal nasal valve angle is the angle between the caudal margin of the upper lateral cartilage and the nasal septum. It normally ranges between 10° and 15°.
Physiology
The dynamics of airflow follows a parabolic curve as air passes through the nasal valve. 4 As a result, contact between the airstream and the mucosal surface is optimized and maximum air-conditioning effects are obtained. The valve may have a role in increasing expiratory resistance and possibly in contributing to air turbulence, which helps in humidification, filtering, and olfaction. This narrow area of the nose functions as the flow-limiting segment. 5
The proper function of the nasal valve is dependent on the integrity of the upper lateral cartilages, the alar cartilages, the mucosal surface of the nasal valve, the nasal septum, and the intrinsic muscles of the nose. 4 The nasal valve can be considered as an inflow regulator. The main resistance to airflow in the entire respiratory tract is normally confined to the nasal valve area.
The physical background for understanding the function of the nasal valve is the law of Poiseuille:

In this formula, V is the volume of passing air through a rigid tube, P1 - P2 is the pressure difference through the tube, r is the radius of the tube; t is the time; η. is the viscosity of air, and L is the length of the tube. When a fixed volume of air passes through a narrowing tube, the pressure will increase in proportion to the decrease in the tube's radius to the fourth power. If the velocity of the air is increased, the pressure will increase across the site of the narrowing. This explains how a nasal valve collapses medially.
Pathology
Anatomic abnormalities at the nasal valve can affect the skin, mucosa, submucosa, muscle, and/or cartilage. It is important to distinguish primary from secondary valve collapse because treating secondary collapse is usually not successful. 2
The primary causes of nasal valve collapse are:
excessive resection of the lower lateral cartilages;
the shape of the lower lateral cartilages;
inherently weak upper and lower lateral cartilages;
an absence of overlap between the upper and lower lateral cartilages;
long returning of the upper lateral cartilages;
soft-tissue stenosis;
facial nerve palsy; and
a narrow piriform aperture. 1
Secondary causes are:
a deviated nasal septum;
a wide columella;
turbinate hypertrophy;
scarring of the vestibular skin;
a slit-like inlet; and
a wide Zuckerkandl tubercle. 1
In this article, we describe our study of quality of life following nasal valve surgery.
Patients and Methods
This retrospective survey was conducted via telephone and based on the Glasgow Benefit Inventory (GBI). 6 Our original study population was made up of 53 patients who had undergone nasal valve surgery at our institution from April 2006 through March 2008. These patients had been referred to us for treatment of a primary complaint of nasal blockage. As part of their assessment, all patients had provided a clinical history and all had undergone a complete ENT examination, including an endoscopic investigation, with particular attention paid to the nasal valve area.
All patients had a positive Cottle sign or modified Cottle sign. Prior to referral, all patients had been prescribed a steroid nasal spray or steroid nasal drops by their general practitioners before being referred to us. Some patients had previously undergone septoplasty and rhinoplasty for nasal obstruction.
Surgical Technique
A variety of methods have been described in the literature to strengthen the nasal valve region and prevent or treat nasal obstruction.3,7–10 When each nasal valve collapse had been diagnosed in our patients, a site-specific surgical technique was carefully planned and individualized to address each patient's specific problem. Surgical considerations that were taken into account were septal deformities and whether the upper lateral cartilage, lower lateral cartilage, and/ or fibroalveolar tissues of the nasal sidewall had collapsed. Butterfly grafts, alar batten grafts, flaring sutures, suspension sutures, and spreader grafts were used as needed. All nasal valve surgeries had been performed by the same surgeon (U.R.).
Glasgow Benefit Inventory
The GBI was specifically designed to evaluate the benefit of ENT procedures. It consists of 18 questions, with six questions in each of three subscale domains: general benefit, physical benefit, and social benefit. Responses to each question are based on a 5-point scale ranging from a large change for the worse (1 point) to no change (3) to a large change for the better (5). Responses to each of the 18 questions are given equal weight, and the mean is transposed to give a GBI score that ranges from −100 (maximum negative outcome) to 0 (no change) to +100 (maximum benefit).
Statistical analysis
All statistical analyses were performed with the Statistical Package for the Social Sciences software (v. 14 for Windows; SPSS; Chicago).
Ethical considerations
As this was a noninterventional audit, ethics committee approval was not applied for.
Results
Of the 53 patients we initially contacted, 39 patients—24 men and 15 women, aged 20 to 50 years (mean: 38)—agreed to participate. Follow-up ranged from 3 to 12 months (mean: 8).
The median total GBI score was +56 (interquartile range: + 32 to + 90.5), and the overall total score was + 58. When we analyzed the individual subscale domains separately, we found that the median scores were + 46 (+ 21 to + 71) for general benefit, + 67 (+ 25 to + 91.5) for physical benefit, and + 50 (+ 17 to + 100) for social benefit (figure 1). The respective overall scores were + 60, + 59, and + 50.
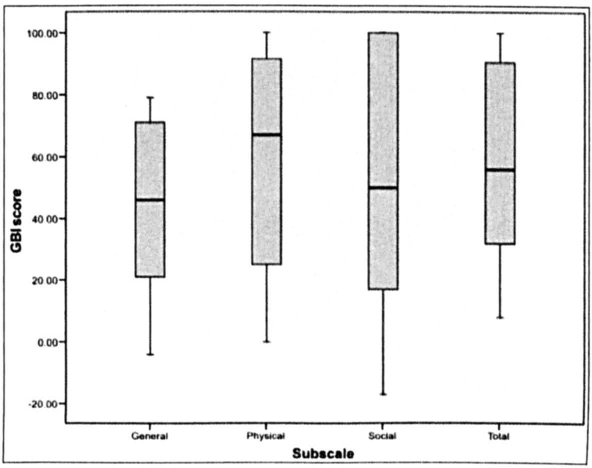
Box and Whisker Plots Show the Median Individual and Total GBI Scores with Interquartile Ranges.
We also analyzed scores separately for women and men (figure 2). For the women, the median total score was + 56 (+ 28 to + 92), and the median subscale scores were + 42 (+ 13 to + 71) for general benefit, + 83 (+ 33.5 to + 91.5) for physical benefit, and + 33 (+ 17 to + 100) for social benefit. For the men, the corresponding scores were + 50 (+ 34.5 to + 89), + 48 (+ 21 to + 71), + 50 (+ 25 to + 91.5), and + 50 (+ 17 to + 75). According to the Mann-Whitney U test, there were no statistically significant differences between the sexes in total benefit (p = 0.765), general benefit (p = 0.831), physical benefit (p = 0.484), and social benefit (p = 0.765). However, the power of the study for determining sex differences was weak.
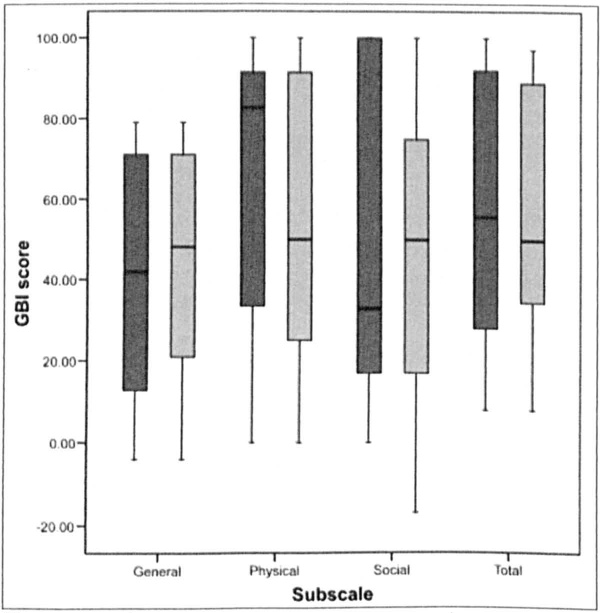
Box and Whisker Plots Show a Comparison of the Various Scores between Women (Blue Bars) and Men (Green Bars).
Discussion
Nasal valve compromise is now recognized as an important cause of nasal airway obstruction. Surgical correction of nasal valve collapse can be effective in reducing nasal obstruction, but the success of the procedure depends on a correct diagnosis and appropriate surgical technique. 11
Outcomes research is now an accepted concept in clinical medicine because it reinforces the fact that the patient plays a central role in modern clinical practice. Quality-of-life questionnaires measure functional capacity, psychosocial well being, and symptomatic relief, which are of utmost importance to patients. The GBI is a useful measure of the degree of benefit patients receive from ENT interventions because it has three important features: it is patient-oriented, it is sensitive to changes in health status resulting from an intervention, and it enables researchers to compare the results of different interventions.
Our review of the literature found no previous study in which the authors used the GBI to assess the quality of life after nasal valve surgery. In 2005, Rhee et al reported their use of the Nasal Obstruction Symptom Evaluation (NOSE) scale to assess quality of life in 20 patients after nasal valve surgery. 12 They concluded that nasal valve surgery improved disease-specific quality of life in patients with symptomatic nasal obstruction and nasal valve compromise.
In our study, the overall total score of +58 clearly suggests that the nasal valve correction was beneficial for our patients. When the three subscale domains were analyzed separately, the improvements were seen in general benefit (+60), physical benefit (+59), and social benefit (+50).
The strengths of our study protocol include the relatively large number of participants (N = 39) and the use of a validated tool. The lack of a nonsurgical comparison group might be considered a limitation of our study, but it is one that is difficult to overcome in a disease process that does not have an acceptable nonsurgical alternative. Also, many patients in our study underwent more than one surgical technique, which makes precise comparisons of the results of each technique difficult to ascertain.
In conclusion, this study suggests that nasal valve surgery plays an important role in symptom control of patients with nasal blockage and that it significantly improves patients’ general, physical, and social quality of life.
Footnotes
Acknowledgments
We thank the staff of the Department of Statistics at the University of Sheffield for their assistance.