
Abstract

Malignancies of the ear and temporal bone are rare and aggressive types of tumors, with a reported incidence of less than 0.2% of all head and neck tumors. 1 These tumors spread mainly by direct invasion into the temporal bone and neighboring structures such as the parotid, infratemporal fossa, dura, and brain. Lymphatic metastases are uncommon, and distant spread is extremely rare.1–3 Ceruminous glands are modified apocrine glands of the external auditory meatus; they rarely give rise to malignant change.2,3
An 85-year-old man with type 2 diabetes presented to the emergency department with a left facial palsy and concomitant symptoms of a chest infection. He was treated with oral antibiotics for radiologically confirmed pneumonia. A diagnosis of unrelated Bell palsy was made by the attending physician, and the patient was also treated with oral steroids and antiviral therapy.
A few weeks later, the patient returned with otalgia and ongoing facial palsy. An otolaryngology review revealed a history of otorrhea and otalgia, but no vertigo or tinnitus. There were no further head and neck symptoms and no history of weight loss.
Examination revealed a large aural polyp occluding most of the tympanic membrane, and the suggestion of a mass behind the eardrum. No perforation could be identified. The patient had a grade VI House-Brackmann facial palsy. The remaining cranial nerves were intact, and there was no cervical lymphadenopathy and no palpable parotid lesion. Findings of flexible nasopharyngolaryngoscopy were unremarkable.
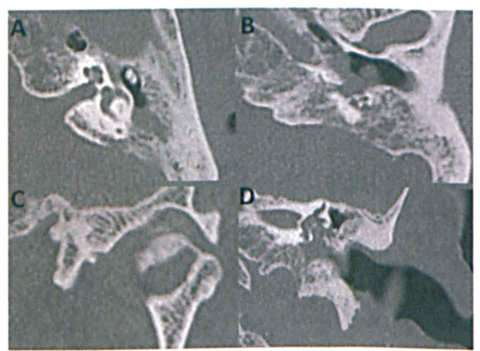
High-resolution computed tomography (CT) of the patient's petrous bones elucidated abnormal soft-tissue density in the left middle ear cavity, with bony destruction (figure 1). At this juncture, given the patient's comorbidities and clinical history, he was treated with topical and intravenous antibiotics along with eye care for likely necrotizing otitis externa.
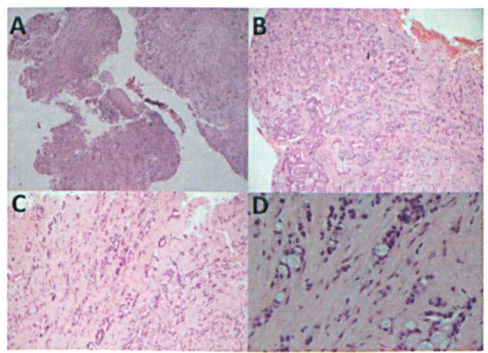
Hematoxylin and eosin stained histopathologic images demonstrate the aural polyp
biopsy at x40
As neoplasia remained a differential, further preoperative imaging and an examination under general anesthesia were performed, with biopsy of the aural polyp. Intraoperative examination highlighted the abnormal nature of the polyp and ear canal tissue.
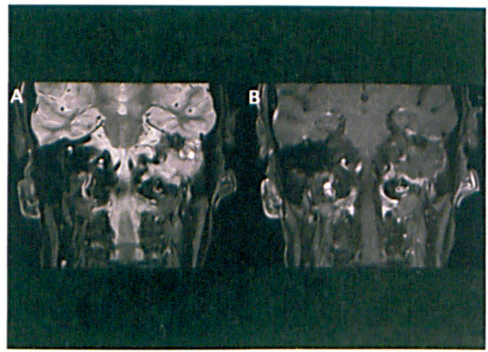
Magnetic resonance imaging (MRI) was suggestive of an infiltrating abnormality (figure 2), and staging CT of the chest, abdomen, and pelvis indicated multiple lytic lesions in the spine and ribs, with a lung mass in the right upper lobe and pleural thickening with signs of resolving infection. Further core biopsies were taken from the chest wall mass.
Histopathology of the left ear polyp confirmed moderately differentiated adenocarcinoma of ceruminous gland origin (figure 3, A and B). The chest wall mass histology (figure 3, C and D), was consistent with the ear canal biopsies and suggestive of metastatic (likely mucoepidermoid) adenocarcinoma of the ceruminous glands of the ear canal. Further staining ruled out a lung, colon, or prostate origin. Prostate-specific antigen and abdominal tumor markers were normal.
Multidisciplinary team discussion and patient deterioration resulted in palliative radiotherapy treatment to the skull base. The patient died shortly thereafter. This case highlights the need to maintain clinical suspicion for neoplasia in necrotizing otitis externa. Nonresolving, dense facial hemiparesis should be further investigated. The exceptionally rare entity of lung metastases secondary to ear pathology should be considered. Ceruminous carcinomas are extremely rare and tend to present as a mass or with otalgia. They are difficult to diagnose histopathologically (in part due to varied and nonstandardized nomenclature). These lesions are thought to respond best to complete surgical excision (if possible, given the complex anatomy of the region) with adjuvant radiotherapy.2,3
Footnotes
Acknowledgment
We thank Dr. Dhafir Al-Okati, consultant histopathologist at Queen's Hospital, for providing the histologic images.