
Abstract
We describe the use of an endoscopic modified Lothrop approach for clearance of an extensive sinonasal-type hemangiopericytoma of the nasal cavity and paranasal sinuses with bilateral frontal sinus involvement in a 44-year-old woman. The modified Lothrop approach is conventionally used to treat sinusitis, but with some slight modifications to the technique, it can also be used for tumor excision.
Introduction
Before the introduction of endoscopic sinus surgery, sinonasal tumors were traditionally excised via open approaches. Although endoscopic sinus surgery was originally intended to address the ostiomeatal complex in sinusitis, 1 its use has extended to other indications, including dacryocystorhinostomy, 2 pituitary gland surgery, 3 and excision of sinonasal tumors. 4 However, an endoscopic approach to large and diffuse tumors of the frontal sinus can be challenging, and therefore these tumors are often addressed by creating an osteoplastic flap. 5 The location of the frontal sinus presents concerns for the endoscopic surgeon in terms of poor visualization, difficult dissection to free the tumor, and suboptimal access for postoperative monitoring for tumor recurrence.
The endoscopic modified Lothrop approach had been well described as a means of managing recalcitrant frontal sinusitis. 6 Although it is usually used to treat sinusitis, with some slight modifications to the technique it can also be used for tumor excision. In this article, we describe our use of this approach to excise an extensive sinonasal hemangiopericytoma involving the left maxillary sinus, the left ethmoid sinus, and both frontal sinuses.
Case Report
A 44-year-old woman presented to our ENT clinic with a 3-year history of intermittent bilateral nasal obstruction, rhinorrhea, and epistaxis. She reported associated discomfort from frontal pressure and pain in the area of the right medial canthus. She denied any symptoms of hyposmia.
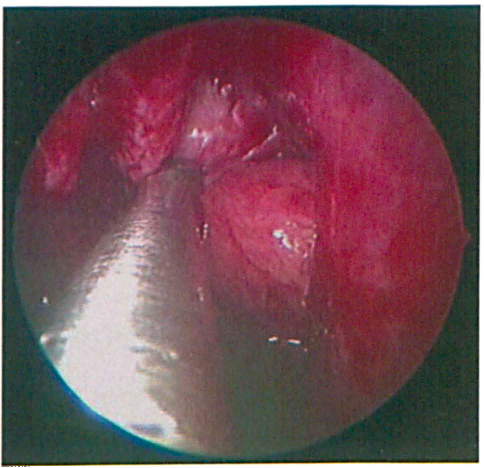
On external examination, a soft prominence was noted in the right medial canthus. Flexible nasoendoscopy revealed the presence of a polypoid mass that had emerged from the left middle meatus and prolapsed into the nasal cavity (figure 1).
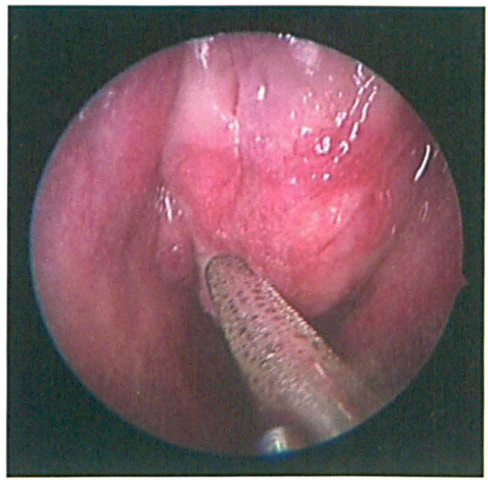
Endoscopic View of the Left Nasal Cavity Shows the Polypoid Mass.
Computed tomography (CT) of the paranasal sinuses demonstrated a heterogeneously enhancing, expansile mass with extensive involvement of the paranasal sinuses (figure 2). In addition to thinning of the anterior skull base, CT showed that the mass was pressing against the crista galli and cribriform plate. The posterior table of both frontal sinuses was intact, but the table on the left side was attenuated (figure 3). No intracranial extension was seen.
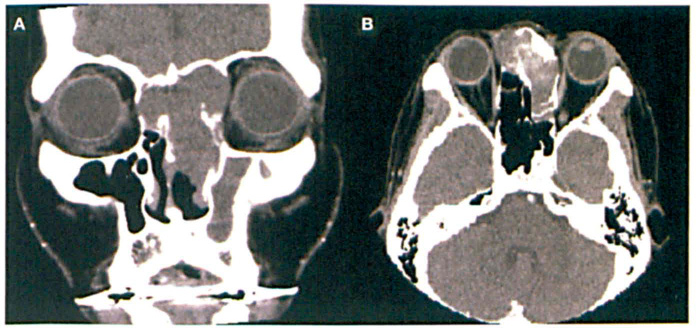
Coronal (
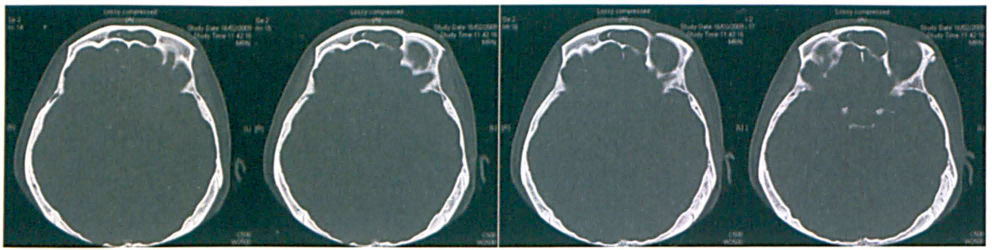
This Series of Axial CTs of the Frontal Sinuses Shows that the Posterior Table of the Left Sinus is Intact but Attenuated.
On magnetic resonance imaging (MRI), the mass was hypointense on T1-weighted imaging (figure 4) and hyperintense on T2-weighted imaging.
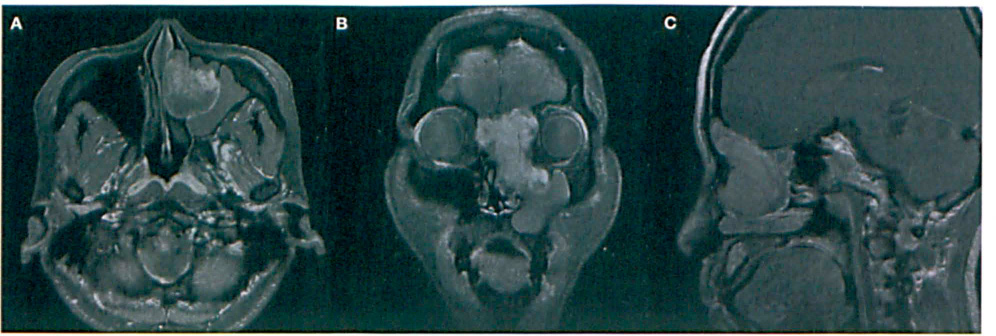
Contrast-enhanced axial (
The differential diagnosis included a slowly growing vascular tumor (possibly a hemangioma) and a neurogenic tumor. Biopsy of the mass suggested the latter.
The patient underwent endoscopic resection of the tumor with image guidance. The large vascular tumor was found to have almost filled the entire left nasal cavity. It appeared to have arisen from the left middle turbinate, and it extended laterally into the maxillary sinus, posteriorly into the anterior ethmoid cells, and superiorly into both frontal recesses and frontal sinuses. The superior part of the nasal septum and the interfrontal part of the septum were eroded, and the soft tissue in the area of the right medial canthus and both laminae papyracea was exposed.
The tumor in the left nasal cavity was debulked and freed from the margins of the enlarged maxillary ostium (figure 5). It was then resected together with the basal lamella and middle turbinate toward the frontoethmoid recess. The basal lamella was resected as it formed the posterior margin of the tumor, and the middle turbinate was resected as it appeared to be the likely origin of the tumor.
Intraoperative Endoscopic Image Shows the Nasal Tumor being Delivered from the Enlarged Left Maxillary Ostium.
An endoscopic modified Lothrop procedure was subsequently performed to access both frontal sinuses. A partial anterior septectomy was performed and extended superiorly to the interfrontal sinus septum that had been eroded by tumor. As both frontal recesses and sinuses were completely filled with tumor, it was not possible to insert the frontal bur to widen the frontal recess. Therefore, we de-bulked the tumor and allowed it to collapse inward while providing space between the tumor and the Walls of both frontal recesses and sinuses. Using the space that was created, we were able to use the bur to widen the walls of these recesses and sinuses. The floor of both frontal sinuses was then removed in the usual manner for a modified Lothrop approach. The tumor was completely dissected from the walls of the frontal sinuses and skull base. The total amount of blood loss by the end of the operation was estimated to be 1 L.
The patient recovered well during the immediate postoperative period, and nasal packing was removed the following day. On subsequent follow-up in the clinic she remained well, exhibiting only mild crusting in the nasal cavities.
Discussion
Sinonasal hemangiopericytoma represents a rare group of vascular tumors of the nasal cavity and paranasal sinuses. Much is still unknown about these tumors. They are believed to arise from pericytes of Zimmermann, which are baroreceptors found on blood vessel walls. 7 Based on published case series and individual reports, sinonasal hemangiopericytomas appear to be slowly growing benign tumors that are associated with a favorable prognosis—unlike the case with their soft-tissue counterparts, which tend to be more aggressive, more destructive, and more likely to metastasize. 8
Sinonasal hemangiopericytomas usually manifest as a unilateral nasal obstruction with epistaxis in patients in the sixth decade of life.7,9–12 They usually appear as a smooth polypoid mass that may bleed on contact. They can arise from any part of the nasal cavity or paranasal sinus.
Surgery is the main treatment modality for sinonasal hemangiopericytomas. A wide range of surgical procedures, ranging from a simple polypectomy to a complete resection with tumor-free margins, has been described.10,11 Recurrence can occur as a result of inadequate surgical excision.7,13
The tumor in our patient was extensive and involved both frontal sinuses. Traditionally, surgical excision of frontal sinus tumors is performed via an open approach. Open approaches include the Riedel, Lynch, and Killian procedures, as well as the osteoplastic flap approach. Among the open approaches, the placement of an osteoplastic flap through a bicoronal incision appears to be associated with the least morbidity. However, issues remain with frontal neuralgia, frontal bruising and edema, and cosmesis. 14
The frontal sinus is the most technically challenging sinus to access, even more so when the surgeon is faced with a diffuse tumor involving both frontal sinuses. Concerns include poor visualization, the inability to dissect tumor from all the sinus walls, difficulty controlling bleeding from vascular tumors, and suboptimal exposure for postoperative tumor monitoring.
The endoscopic modified Lothrop approach was first described by Gross et al in 1995 15 and later popularized by Wormald 6 for the treatment of recalcitrant frontal sinusitis. In such patients, the technique involves creating a septectomy so that both middle turbinates and their axillae can be seen in the same endoscopic view. The surgeon then identifies both frontal recesses and sinuses. These are first widened and drilled anteriorly and laterally, and then they are drilled medially to join both the frontal sinusotomies.
The surgical treatment of tumors, particularly vascular tumors such as sinonasal hemangiopericytomas, is certainly more challenging than the treatment of sinusitis in terms of blood loss. Tumor removal is different from sinusitis treatment in other ways:
Tumor can fill the middle meatus and obstruct access to the frontal recess.
Tumor can fill the frontal recess and prevent effective drilling with a bur.
Unlike the typical scenario in which the surgeon sees both frontal recesses and simply joins the floor of both frontal sinuses by dissecting medially, the margins of dissection are filled with tumor and there is no obvious cavity.
Since the frontal sinus is filled with tumor, the dimensions of the frontal sinus cavity cannot be visualized. There is a reduction in depth perception and an increase in the risk to adjacent areas, especially the orbit and posterior wall of the frontal sinus.
The surgical approach requires that the tumor be debulked from the lower sinonasal cavities to expose the bilateral tumor-filled frontal recesses. The usual septectomy should still be performed, and tumor in the frontal recess needs to be debulked from “within,” like removing the core from an apple. This allows the surgeon to dissect the walls of the tumor away from the sinus walls so that the walls of the tumor collapse inwardly.
Once the tumor walls collapse, space is created for the safe entry of the bur between the tumor and the walls of the frontal recess, particularly the frontal beak, thus allowing for widening of the frontal recess. The frontal sinuses are joined—not from frontal recess to frontal recess, but from tumor to tumor, from one side to the other. In these cases, image guidance improves three-dimensional perception and compensates to some extent for the lack of depth perception. It also helps determine the limits of safe dissection.
Although we did not use preoperative embolization, it should certainly be considered when preoperative investigations suggest a vascular tumor. A greater palatine block should be performed to minimize blood loss. This is the only effective method of local infiltration in the presence of a large tumor that has filled the sinonasal cavity. 16
Debulking a tumor with the assistance of a micro-debrider is useful as the continuous suction provides good visualization. Using standard instruments such as Blakesley forceps and Tru-Cut forceps is too slow a process, and the pooling blood would prevent further progress. Open, raw areas of tumor, such as the lower border of the remnant tumor after debulking, require hemostasis with bipolar diathermy to minimize blood loss. Finally, the use of suction instruments can be extremely useful by allowing the surgeon to continue dissecting tumor away from the sinus walls in the presence of blood.
In conclusion, we have described the use of the endoscopic modified Lothrop approach for clearance of extensive sinonasal hemangiopericytoma of the nasal cavity and paranasal sinuses with bilateral frontal sinus involvement. In general, the endoscopic approach results in less morbidity than do external open approaches, and yet it provides good access for complete tumor resection and easy postoperative surveillance of the frontal sinus cavity without the need for frequent imaging studies.
Although the incidence of recurrence and metastasis may be low, the biologic behavior of sinonasal hemangiopericytomas remains difficult to predict, and therefore lifelong surveillance is recommended.