
Abstract

A 56-year-old African-American man presented to the emergency department with dyspnea and dysphagia with drooling. On his initial evaluation, disproportionate obesity of the face, neck and shoulders was noted. The patient's history was significant for obstructive sleep apnea, end-stage renal disease, alcoholic liver disease, pulmonary hypertension, and alcoholic cardiomyopathy. He had a multidecade history of heavy alcohol abuse but had quit drinking 2 years previously.
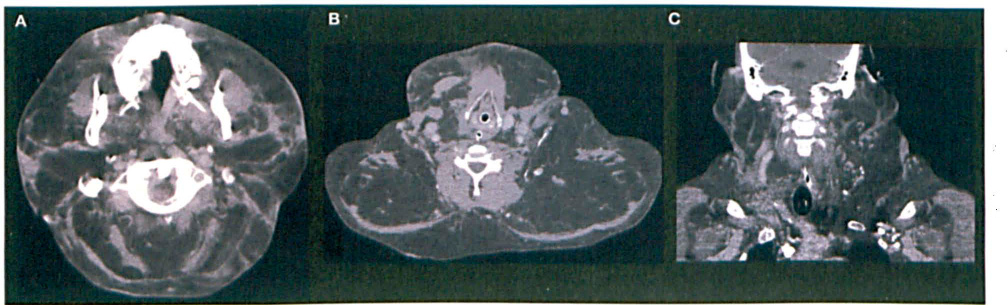
Computed tomography (CT) of the soft tissue of the head and neck showed symmetric, nonencapsulated adipose deposits in the buccal, posterior cervical neck, and axillary regions, with significant oropharyngeal narrowing (figure). No compression of the trachea was seen. Further discussion with the patient revealed that the masses in his head and neck had been growing slowly over the previous 3 years and had been demonstrated on previous images. The adipose deposits, sparing the distal extremities in this patient, were consistent with so-called multiple symmetric lipomatosis (MSL), also known as Madelung disease.
This condition occurs primarily in men and is strongly associated with a history of alcoholism. 1 The pathogenesis is not fully understood, but recent evidence suggests that MSL results from defective noradrenergic regulation of mitochondria in brown fat.2,3 Notably, the distribution of excessive adipose tissue in MSL mirrors the distribution of brown fat found in infants.
The course of the disease typically involves slow, progressive growth of the adipose deposits. Patients with MSL commonly also suffer from various neuropathies, especially paresthesias and autonomic neuropathy. These neuropathies do not correlate with alcohol intake but are believed to be an intrinsic aspect of the disease process. 4 MSL is also associated with hyperuricemia and sleep apnea.4,5
The most effective treatments for MSL are surgical: lipectomy, liposuction, or ultrasound-assisted liposuction. 6 Treatment indications include: sleep apnea, aerodigestive tract compression, neck pain, and/or aesthetics. Alcohol cessation may help stop the progression of lipomatosis, but regression is rare. Even patients who cease alcohol intake or who were never alcoholics may see progression of the disease.2,4
Our patient's presentation with MSL was notable in that he was African-American. Only one case of MSL previously has been described in an African-American. 7 MSL is believed to be most common in males of Mediterranean descent. 4 Additionally, while our patient's history of alcoholism and liver disease is consistent with past reports of MSL, his clinical presentation was complicated by his end-stage renal disease, pulmonary hypertension, and cardiomyopathy.
The patient's acute dyspnea and dysphagia resulted from airway compression due in part to the size of his facial and anterior cervical adipose deposits. A sleep study was warranted because his oropharyngeal compromise was the cause of his sleep apnea, and sleep apnea is a known complication of MSL.4,5 The presence of apnea could have contributed to his pulmonary hypertension.
There is often a long delay before the diagnosis of MSL, which is often confused with obesity. However, MSL is a distinct clinical entity from obesity. Diagnosis is made clinically, based on the distribution of adipose tissue, as well as the patient's sex, age, and history of alcohol use. CT or magnetic resonance imaging can confirm the presence of symmetrical, unencapsulated fat deposits in the presurgical stage. 8