
Abstract
An otherwise healthy 13-month-old girl was noted by her pediatrician to have developed a left head turn. The patient was referred to a pediatric ophthalmologist, who noticed signs of incomplete third cranial nerve palsy, Magnetic resonance imaging revealed the presence of an abnormal lesion in the inferonasal orbit that was abutting the ethmoid sinus. After consultation with an ENT specialist, the decision was made to remove the lesion via functional endoscopic sinus surgery because this approach was deemed to provide adequate access while limiting morbidity. Histology of the excised lesion identified it as true ectopic lacrimal gland tissue with cysts. We recognize and comment on the fact that in many reported cases of ectopic lacrimal gland cyst, the tissue was not ectopic at all but instead represented an extension of normal lacrimal gland tissue.
Introduction
Pseudo third cranial nerve (CN III) palsy and cysts of the ectopic lacrimal gland are both very rare entities.1,2 True ectopic lacrimal gland tissue is distinct lacrimal tissue found outside the lacrimal gland fossa. 3 This phenomenon is rare, and it is usually found incidentally. 4 Ectopic lacrimal gland tissue may present as a solid or cystic mass, and it usually causes globe displacement. 5 A cyst of the lacrimal ducts can occur in any location where lacrimal gland tissue is present. 3
A variety of diseases involving the orbit can lead to ptosis and disturbed eye movements. However, if the neuronal pathways are not disturbed, the condition is not considered to be a true CN III palsy.2,6Instead, it is referred to as pseudo third cranial nerve palsy. Restrictive myopathies and diseases of the neuromuscular junction are responsible for most pseudo CN III palsies. 2
We report a new case of pseudo CN III palsy in a very young child with a true orbital ectopic lacrimal gland cyst that was successfully removed via functional endoscopic sinus surgery (FESS).
Case Report
An otherwise healthy girl who had been born after an uncomplicated pregnancy was noted by her pediatrician to have developed an unusual head posture at 9 months of age, as her face was constantly turned left of midline. At the age of 13 months, she was seen by a pediatric ophthalmologist, whose examination found a steady and maintained gaze in both eyes in addition to the prominent left head turn (figure 1, A), a position that is often adopted by a child with ocular muscle misalignment to avoid double vision. The patient demonstrated marked deficits in motility in the right eye and a prominent right exotropia (outward deviation of the globe) in primary gaze, which was indicated by the corneal light reflex (figure 1, B). The motility of the left eye was normal.

At presentation, the patient exhibits the marked left head turn
(
The ocular examination was also remarkable for anisocoria (differently sized pupils), as the pupil of the right eye was larger than that of the left eye in both light and dark settings. However, both pupils were briskly and equally reactive to light without any afferent defect. The examination showed no ptosis, proptosis, or periocular fullness. Findings on a complete anterior and posterior segment examination of both eyes were unremarkable. The patient had no history of trauma or surgery and no significant family history of ocular disease. Her outward signs mimicked those of CN III palsy.
Magnetic resonance imaging (MRI) of the orbits with gadolinium contrast detected a smooth, oval, well-circumscribed, minimally enhancing, extraconal tumor in the inferonasal right orbit (figure 2). The mass was located on the nasal side of the medial rectus muscle, and it abutted the ethmoid sinus. No signs of bony destruction were evident. The lesion demonstrated tissue characteristics similar to those of vitreous on both T1- and T2-weighted imaging.
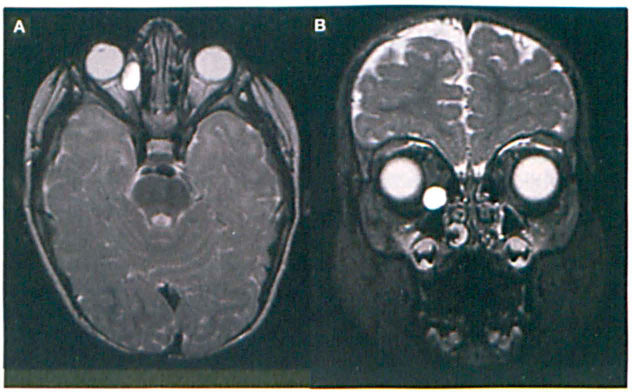
Gadolinium-enhanced axial (
An excisional biopsy was discussed with the family. Our initial recommendation was for a direct medial orbitotomy, but the family was extremely concerned about cosmesis and complications. Further review of the MRI films suggested that the tumor might be amenable to removal via an endoscopic sinus approach. An ENT consultation was obtained, and an attempt to remove the tumor via FESS was planned. An orbital surgeon was present during the planning in case a direct orbitotomy would be needed.
In the operating room, FESS was performed with a right total ethmoidectomy and removal of the right medial orbital wall. As the right medial periorbita was opened, a tense, thin-walled, fluid-filled mass that measured approximately 8 × 12 mm herniated into the ethmoid sinus. The mass was then removed in toto transnasally.
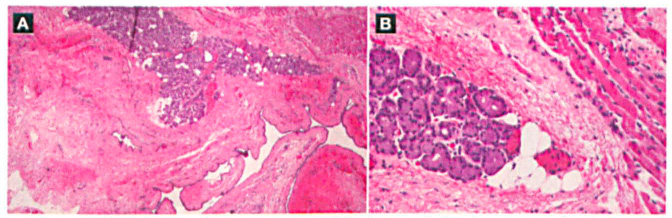
Histopathology of the specimen identified a large cyst lined with a layer of bland cuboidal epithelium (figure 3). The cyst was directly adjacent to a small area of aberrant lacrimal gland tissue, which lay between the cyst and a small portion of skeletal muscle. No inflammation or atypia was seen in any of the resected tissue.
Although the surgery did not correct the patient's left head turn, she remained asymptomatic for more than 2 years with no tumor recurrence.
Discussion
Ectopic lacrimal gland tissue has been reported in the eyelid, conjunctiva, sclera, cornea, iris, orbit, choroid, and nasal mucosa.1,2,4,5 Unfortunately, much of the reporting in the literature has been both confusing and inaccurate. In fact, most reported cases of ectopic lacrimal gland tissue did not truly involve lacrimal gland tissue that was separate and distinct from the lacrimal gland fossa, which suggests that those lesions were not ectopic.
For example, Garrity et al described an anterolateral orbitotomy in which they encountered lacrimal gland tissue that extended posteriorly toward the orbital apex. 4 While they described this tissue as ectopic, it was not. Instead of true ectopic tissue, these misreported cases actually involved a posterior extension and enlargement of the normal lacrimal gland to accommodate a cyst, an inflammatory lesion, or a neoplasm. Therefore, these cases should not be considered examples of ectopic lacrimal gland tissue. Many other authors share our opinion that most lacrimal gland lesions from the superotemporal area of the orbit are not truly ectopic. 3
Cyst formation may occur in any location where lacrimal gland tissue is present. 7 The mechanism of ectopic lacrimal gland with cyst formation is unclear. Some authors have theorized that a kinking of the lacrimal gland duct results in stasis of the secretory products.3,5
Typically, a progressively enlarging intraorbital cystic mass would be expected to cause a progressive unilateral proptosis, but this did not occur in our patient. Her extra-axial tumor produced an unusual clinical appearance of a pseudo CN III palsy. True CN III palsies occur as a result of pathologies that affect the neuronal pathways of CN III. 8 Possible causes include ischemia, demyelinating lesions, infection, and aneurysms, but the specific pathology varies with the anatomic course of the nerve. True CN III palsies can present with some or all of the following deficits: vertical and horizontal diplopia, ptosis, a down-and-out position of the affected eye, and mydriasis. On the other hand, pseudo CN III palsies are typically caused by pathologies that involve the orbit or extraocular muscles in a more mechanical fashion, which leads to a clinical presentation that may include only one or two of these deficits.
The pseudo CN III palsy in our patient was likely attributable to mechanical factors (e.g., muscle restriction and compressive effects) that caused maldevelopment of the medial rectus muscle and secondary strabismus. We believe the mydriasis occurred secondary to the mass effect, which impaired the function of the parasympathetic pupilomotor fibers.
FESS has become an ideal method of managing certain orbital complications. 9 In children, the use of an endoscopic approach to manage orbital subperiosteal abscesses and orbital floor fractures has been shown to be a valuable surgical modality.10,11 We have not encountered any reports in the literature in which the authors suggested using an endoscopic approach for tumor removal specifically in children. FESS carries the advantages of providing excellent visualization while minimizing cosmetic defects and functional morbidity. 9 Our case lent itself to this approach because the tumor was fairly deep and it rested directly against the medial orbital wall.
We caution that the removal of an orbital tumor in a child via FESS should be performed only by an experienced sinus surgeon. This approach can be particularly challenging in view of the limited amount of space in a child's sinuses, difficulty with complete dissection around the tumor, and the complexity involved in delivering a large mass through a small pediatric nostril.
In summary, we strongly recommend orbital imaging in any child with progressive proptosis, strabismus, or apparent CN III palsy. In the event that a cystic mass is identified, consideration of the possibility of ectopic lacrimal gland tissue should be included in the differential diagnosis. Multiple options for surgical management of pediatric orbital tumors should be entertained, including FESS in select cases.