
Abstract
We describe the case of a 24-year-old man who underwent open septorhinoplasty for the treatment of progressive nasal disfigurement caused by a nasal hump. Postoperative histopathology of the resected hump revealed that it was an osteochondroma. The patient showed no evidence of recurrence during 2 years of follow-up. To the best of our knowledge, this is the first case of an osteochondroma involving the nasal dorsum to be reported in the English-language literature.
Introduction
Cartilaginous tumors are rare in the head and neck region. Chondromas are slowly growing asymptomatic tumors that are usually discovered incidentally. An osteochondroma can be considered a cartilage-covered osseous excrescence that arises from the surface of a bone. Osteochondromas occur as both multiple (hereditary multiple exostoses) and solitary lesions. Some arise spontaneously and others after an injury or exposure to radiation.
Osteochondromas represent 36% of all benign bone tumors. 1 The most common sites are the long tubular bones, especially the femur, humerus, and tibia. 1 In the maxillofacial region, they are most common in the mandible, the condylar area, and the tip of the coronoid process. 2 To the best of our knowledge, involvement of the nasal bone has not been previously described. We report what we believe is the first such case.
Case Report
A 24-year-old man was evaluated for a history of nasal obstruction and progressive nasal disfigurement. He reported that a hump in his nasal dorsum had progressively increased in size over the previous 4 years. He had no history of relevant trauma, infection, or exposure to radiation. The clinical examination revealed the presence of a disfiguring nasal hump (figure 1). Computed tomography of the paranasal area was not diagnostic for a specific disease.
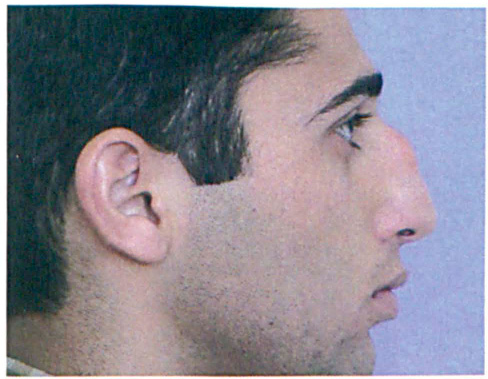
Photo shows the preoperative nasal profile.
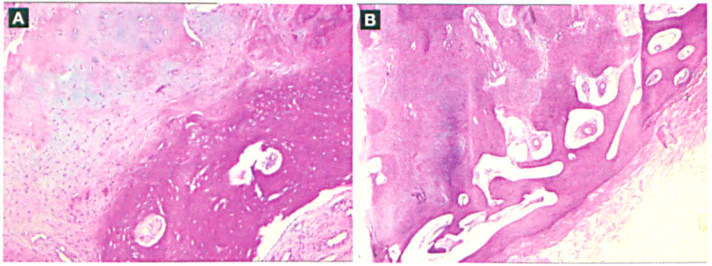
The patient underwent an open septorhinoplasty to remove the hump. Intraoperatively, it was noticed that the osteochondral junction of the nasal dorsum was not smooth, that there were some adhesions between the nasal dorsum and the subcutaneous tissue, and that the keystone area was very soft. Postoperatively, histopathologic assessment of the resected nasal hump identified it as an osteochondroma (figure 2).
Two years postoperatively the patient was doing well, and no recurrence was detected during follow-up. The cosmetic result was satisfactory (figure 3).
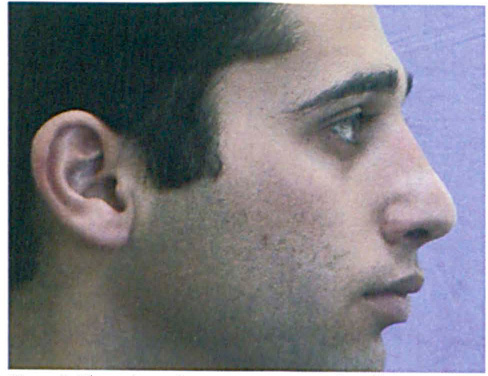
Photo shows the postoperative nasal profile.
Discussion
Osteochondromas are predominantly osseous. They are produced by a progressive endochondral ossification of a growing cartilaginous cap. An osteochondroma can occur in or on any bone where endochondral ossification occurs.
Osteochondromas commonly arise along the side of tendon insertions, with the direction of growth following the line of the tendinous pull.1,2 Brady et al 3 found evidence to support the theory of histogenesis offered by Lichtenstein 4 to explain the presence of osteochondromas in extracondylar locations in which tendon insertions are not present. They suggested that all periosteum has the pluripotentiality to give rise to cartilaginous as well as osseous cells.
Most osteochondromas are located at or near the epiphyseal-metaphyseal junction of the long bones, especially at the lower metaphysis of the femur and the upper metaphysis of the tibia. They are also seen in the ilium, scapula, and vertebrae. 1 Dahlin and Unni reported in a review of 640 cases of osteochondroma that approximately 88% of those patients had a solitary lesion. 1
Osteochondromas are usually found in young patients (60 to 80% of patients with these tumors are younger than 21 years of age), and there is no predilection for either sex. 1 The most characteristic clinical manifestation is a slowly growing, painless mass. 5 The growth of the tumor usually parallels that of the patient, and the lesion often becomes quiescent when the epiphyses have closed.
While osteochondromas are benign lesions, malignant transformation does occur in almost 1% of cases.1,6 Such transformation usually manifests as a chondrosarcoma.1,6 As far as we know, only 1 case of a secondary chondrosarcoma arising in an osteochondroma of the nasal septum has been reported. 6 In our case, no sarcomatous change was detected on histopathologic examination. Also, microscopic examination found no evidence of invasion of surrounding tissues and no atypical cells.
Many osteochondromas are asymptomatic and therefore escape detection. However, they occasionally lead to significant symptoms and signs related to a fracture of an exostosis and damage to the adjacent nerves or vessels. Dahlin and Unni considered the presence of an osteocartilaginous exostosis insufficient reason for surgical extirpation because malignant transformation is so rare. 1 Surgical removal is indicated (1) if the tumor is unsightly, painful, or disabling, (2) if its radiologic features are suggestive of a malignancy, or (3) if it shows an abnormal increase in size.1–3,7