
Abstract
Electrical injuries can occur as a result of contact with low- or high-voltage electricity. Low-voltage injuries are more common, as they usually occur in the home, but reports in the literature are few. After exposure to electric current, almost every organ system in the body is affected. The severity of an injury depends on many factors, including the type of current, the duration of exposure, and the resistance of the tissue involved. Reported cases of hearing loss and facial nerve paralysis associated with low-voltage electrical shock are rare, and minimal information is available about this circumstance. In this article, the author describes a case of low-voltage electrical shock in a 20-year-old man. To the best of the author's knowledge, this is the first report in the literature of a resolution of unilateral sensorineural hearing loss and facial nerve paralysis caused by a low-voltage electrical shock.
Introduction
Electrical shock is a relatively uncommon form of trauma, and reports in the literature are relatively sparse. In 1997, Cherington et al reported that in the United States, electrical shock was responsible for 7% of all deaths due to job-related trauma. 1
The severity of electrical shock injury depends on many variables: the type of current, the duration of exposure, the resistance of the tissue involved, the level of applied voltage, the contact surface area of the body, involvement of water or metal, and the path that the current takes through the body.2,3 In the medical literature, electrocutions are typically categorized according to the level of applied voltage as low-voltage (<1,000 V) and high-voltage (≥1,000 V). 4 Low-voltage injuries are more common, as they usually occur in the home. In this article, the author reports a new case of low-voltage electrical shock that caused hearing loss and facial paralysis.
Case Report
A 20-year-old man with no significant medical history was attempting to repair a refrigerator at his home. With the refrigerator still plugged into the electrical outlet, he attempted to strip an electrical cable with his teeth. He received a low-voltage electrical shock (230 V, 50 Hz) for an unknown duration of time. He had several metallic dental fillings.
Witnesses reported that at the time of the shock, the man jerked backward and lost consciousness, but he did not exhibit seizure activity. The man later reported a feeling of confusion, a metallic taste in his mouth, inability to close his left eye, and left-sided hearing loss. The appearance of his face was asymmetric, and his speech was slurred.
The man was taken to our otolaryngology clinic. Physical examination confirmed his facial asymmetry (figure 1, A) and his inability to close his left eye. It also revealed that he was unable to whistle or pucker the left side of his lips (figure 1, B). The patients other cranial nerves were intact, and no cerebellar deficits were noted. His tympanic membranes were intact bilaterally, and no hemotympanum was seen. Audiometry revealed a left-sided sensorineural hearing loss (figure 2, A).
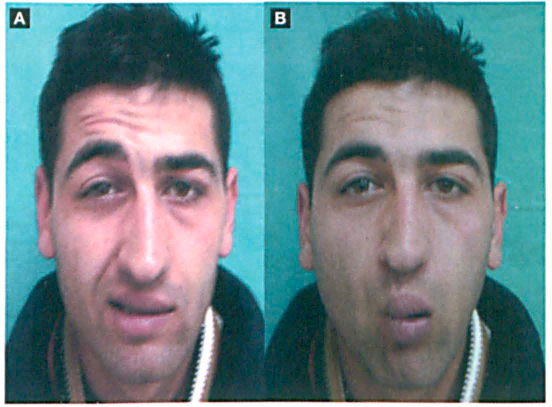
At presentation, the patient is unable to move the left side of his face
(
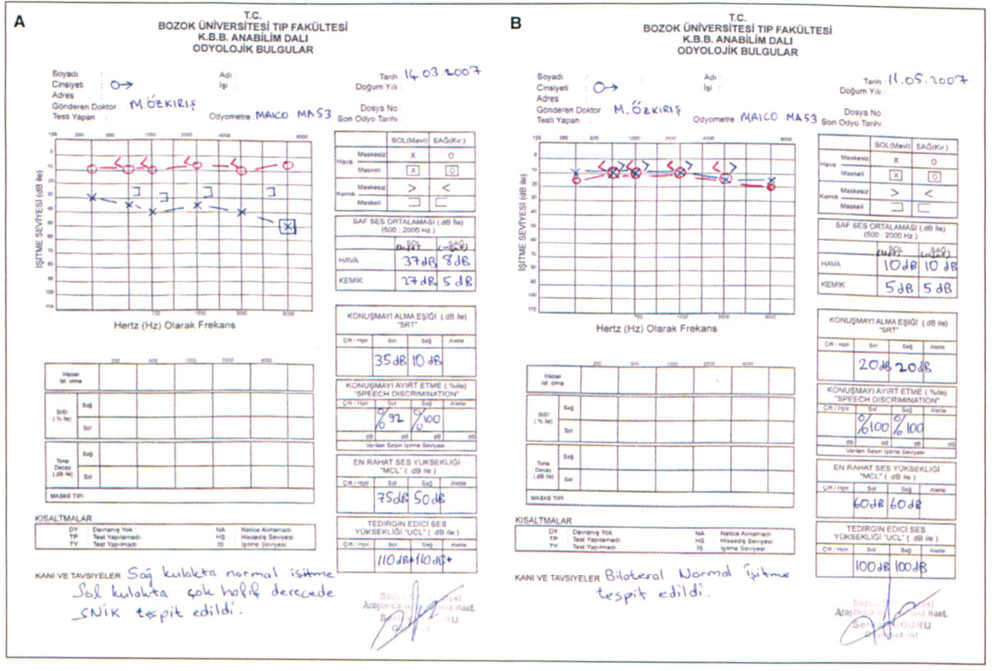
Audiograms document the left-sided sensorineural hearing loss
(
To treat the hearing loss and facial paralysis, the patient was administered a single injection of prednisolone (250 mg) and prescribed a tapering dose of oral prednisolone for 12 days. At 2 months of follow-up, his hearing had improved (figure 2, B) and his facial paralysis had resolved.
Discussion
After exposure to electric current, almost every organ system in the body is affected. The human body is a good conductor of electricity, and direct contact with electric current can be fatal. While some electrical injuries may appear to be outwardly minor, serious internal damage might be present, especially injury to the heart, muscles, and brain.5,6
Many complications of low-voltage electrical shock have been reported; they include seizures, transient quadriplegia, hemiplegia, hemiparesis, general motor weakness, reflex sympathetic dystrophy, ventricular fibrillation, abdominal visceral injuries, scapular fracture, and carpal tunnel syndrome. Moreover, rare occurrences of delayed-onset and chronic sequelae secondary to low-voltage electrocution have been documented; such sequelae include amyotrophic lateral sclerosis/motor neuron syndrome and impotence. 7
In high-voltage injuries, loss of consciousness may occur, but it is usually transient unless there is a significant concomitant head injury. Prolonged coma with eventual recovery has also been reported. Patients may exhibit confusion, a flat affect, and difficulty with short-term memory and concentration.8,9
Electrical injury to the central nervous system may cause seizure, either as an isolated event or as part of a new-onset seizure disorder. Other possible reasons for a seizure following electrical shock, such as hypoxia and traumatic central nervous system injury, should also be considered. Neurologic symptoms may abate, but long-term disability is common. Lower-extremity weakness is commonly undiagnosed until ambulation is attempted. 10
The head is a common point of contact for electrical shocks, and patients may exhibit burns there as well as neurologic damage. Cataracts can develop in approximately 6% of patients who have sustained an electrical injury, and therefore they should be suspected whenever an electrical shock has occurred in the vicinity of the head. 11 Cataracts may arise immediately or shortly after the accident, but they more typically begin to appear months after the injury. Visual acuity and fundus examinations should be performed at presentation or as soon as practical for documentation.
Tympanic membrane rupture is not common after electrical injuries; when it does occur, it may be caused by a shock wave's direct burn or by a basilar skull fracture. Although most patients recover without serious sequelae, disruption of the ossicles and mastoid bone may occur, as well as cerebrospinal fluid otorrhea, hemotympanum, and permanent deafness.2,3
Although most low-voltage electrocutions result in minor ephemeral complications, the case presented here was marked by unilateral sensorineural hearing loss and facial paralysis. The patient's recovery after treatment with steroids can lead us to believe that the mechanism that produced these sequelae was the damage to the central nervous system caused directly by the electricity itself. To the best of the author's knowledge, this is the first report in the literature of a resolution of unilateral sensorineural hearing loss and facial nerve paralysis caused by a low-voltage electrical shock.