
Abstract

A 52-year-old woman presented with a 6-month history of dysphonia. Flexible laryngoscopy demonstrated a hemorrhagic polyp on the superior aspect of the left true vocal fold. Based on the unusual location of this mass outside the vibratory margin, videostroboscopy was performed. It confirmed the presence of the mass, as well as diffuse stiffness and infiltration of the left true vocal fold. The right true vocal fold also had irregularity of the vibratory margin (figure). Based on these findings, it was determined that an infiltrative, possibly infectious, process was present. A chest x-ray was performed and infectious disease consultation obtained. Sputum cultures performed by infectious disease confirmed the presence of acid-fast bacilli.
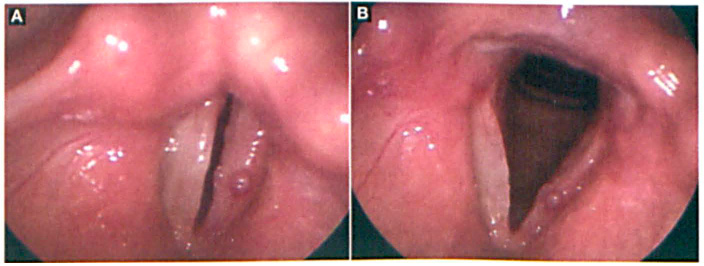
Videostroboscopy shows vocal folds in the adducted position (
Laryngeal tuberculosis is a rare, highly contagious disease. Its incidence has been on the rise worldwide since 1993. This increase is primarily attributed to the AIDS epidemic, increased poverty, drug addiction, and decreased immunization coverage.1,2 Because of its uncommon clinical presentation, laryngeal tuberculosis is often confused with chronic laryngitis and laryngeal carcinoma. Diagnosis is often delayed because of its nonspecific symptoms and its ability to mimic other diseases.
Presenting symptoms include hoarseness, hemoptysis, dysphagia, dysphonia, dyspnea, and odynophagia. The pathogenesis of laryngeal tuberculosis can be primary or secondary in origin. It is more frequently a secondary complication of pulmonary tuberculosis.3,4
The diagnosis of laryngeal tuberculosis is often suspected clinically, but in patients with less specific symptoms, flexible laryngoscopy may reveal only an inflammatory picture. Videostroboscopy may further delineate the extent of involvement in subtle cases. Findings on videostroboscopy may include decreased mucosal wave, vocal fold scarring disproportionate to the visible lesion, vibratory margin irregularities, and bilaterality of abnormalities in the face of a unilateral lesion.
Antituberculous therapy including rifampin, isoniazid, pyrazinamide, and ethambutol offers a good prognosis for patients, generally curing the disease without any sequelae. The response of laryngeal tuberculosis to treatment is rapid, with pain relieved within a few days.