
Abstract
A 70-year-old woman was referred to us for evaluation of a presumed left-sided neck mass. The referral was based on the visual appearance of subtle neck asymmetry. The patient reported no ENT symptoms. Clinical examination and ultrasonography identified no pathology, but computed tomography revealed that the asymmetry was present because the patient's right sternocleidomastoid muscle (SCM) was absent. The SCM on the left side was normal. Congenital absence of an SCM is uncommon, and to the best of our knowledge, an initial presentation in an adult has not been previously reported in the literature.
Introduction
The congenital absence of a sternocleidomastoid muscle (SCM) has been traditionally described in pediatric patients, and it is associated with congenital torticollis. 1 We describe a case in which the absence of an SCM was not detected until the patient was an older adult.
Case report
A 70-year-old woman was referred to our ENT Department for evaluation of a presumed left-sided neck mass. The physicians presumption was based on the visual appearance of subtle neck asymmetry, which was noticed while the patient was being evaluated for an unrelated complaint. The asymmetry could not be characterized on clinical examination, and ultrasonography identified no pathology. Therefore, the referral was made.
On direct questioning, the patient said she had not noticed any neck mass, and she experienced no associated sinister symptoms such as weight loss, dysphagia, or hoarseness. She did not abuse alcohol or smoke cigarettes. Visual inspection revealed no obvious asymmetry, but clinical examination did identify a left-sided neck “mass” at level III-IV; this mass was fixed, diffuse, and nontender. Findings on the remainder of the ENT examination, which included flexible nasoendoscopy, were normal.
Computed tomography (CT) was obtained, and it showed that the asymmetry was attributable to the absence of a right-sided SCM; the left side of the neck was completely normal (figure). No other abnormalities were detected, and no further action was required.
Discussion
The congenital absence of an SCM is rare, as only a few cases have been described in the literature. Its pathogenesis is unknown; in addition to a genetic cause, theories involving inflammatory, vascular, neuropathic, and myopathic insults during embryogenesis have been suggested.1,2
The SCM acts alone in allowing the head to tilt to the side, and therefore a congenital absence of an SCM is associated with congenital torticollis. 3 Our patient presented at a late age, and she had a full range of neck movements without torticollis.
The absence of an SCM leaves a potential space through which the lung can herniate. Because lung herniation can lead to incarceration, surgical correction of the deformity may be required. 4
The late presentation in this case was likely attributable to the fact that the neck asymmetry was not obvious on visual inspection. We can assume that a compensatory overgrowth of soft tissue in the affected side of the neck over many years made the asymmetry less than obvious.
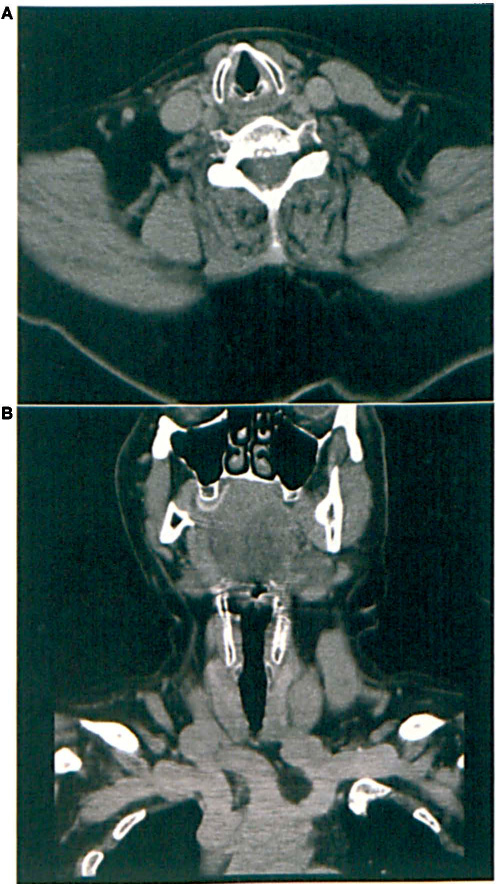
Axial (
The unilateral absence of an SCM may be suspected on ultrasonography of the neck, but interpreting such images in infants can be difficult. The emphasis is on the identification of symmetrical structures, but in cases of torticollis, inspection of the images of the abnormal side may be limited because of the position of the neck. CT is the investigation of choice when a malignancy is suspected, but the risks of delivering radiation to children must be taken into consideration, and magnetic resonance imaging may be more appropriate in these cases.
In cases of congenital torticollis, conservative treatment includes stretching, physiotherapy, and fitting with a neck brace. In some circumstances, surgical release of the fibrotic area of the SCM may be required. In cases of complications such as lung herniation, the defect may be corrected with fasciocutaneous and myocutaneous flaps, which would also correct the cosmetic deformity. 4
In conclusion, the congenital absence of an SCM is rare, and such an initial presentation in an adult has not been previously reported. The pathogenesis of an absent SCM is unknown, but a genetic cause and inflammatory, vascular, neuropathic, and myopathic events during embryogenesis have been postulated. Our case highlights the importance of the inclusion of embryologic abnormalities in the differential diagnosis of an apparent neck swelling.