
Abstract

Polymorphous low-grade adenocarcinoma (PLGA) is a low-grade malignant epithelial tumor characterized by an infiltrative growth of cytologically uniform cells arranged in a multitude of architectural patterns. While it is an uncommon tumor, it accounts for about 25% of all intraoral minor salivary gland malignancies. Most patients come to clinical attention between the ages of 50 and 70 years, and the female-to-male ratio is 2:1. PLGA has a predilection for blacks.
PLGA is exclusively a tumor of the minor salivary glands. It affects the palate (60% of cases) most commonly, especially at the mucosal junction of the hard and soft palates; the next most common sites are the cheek and the lip, often the upper lip. PLGA generally appears as a nodule or nontender mass; some patients complain that their dentures no longer fit correctly. The tumor may be mobile or fixed, depending on the duration of symptoms (as long as 40 years). Complete yet conservation excision is recommended, although perineural proclivity may dictate making a slightly wider resection margin. Patients with PLGA generally have an excellent long-term clinical outcome (10-year survival: ∼95%). Recurrences are seen in as many as 15% of cases, usually within 5 to 7 years of treatment of the primary tumor; recurrences are more common in women than in men.
PLGAs are usually unencapsulated, firm to solid masses that are covered with an intact squamous mucosa in most cases. They are generally small (mean: 2 cm); tumors of the lip are usually smaller. Histologically, PLGAs are characterized by the widely infiltrative growth of an architecturally diverse but cytologically uniform cell population set within a focally myxoid stroma. The tumor surrounds and entombs the associated minor mucoserous salivary glands and invades the surrounding soft tissues, exhibiting a characteristic “targetoid appearance” around nerves (figure 1).
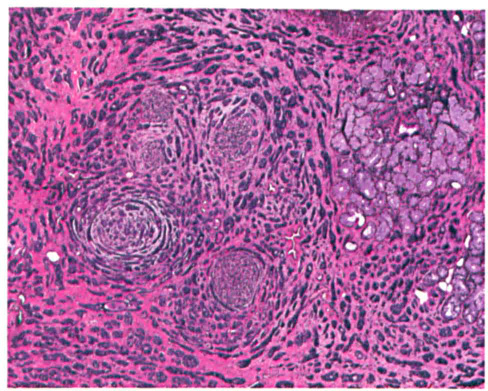
This PLGA exhibits a remarkably complex architecture with encasement of the minor mucoserous glands (right) and the characteristic targetoid growth around the peripheral nerve twigs (center).
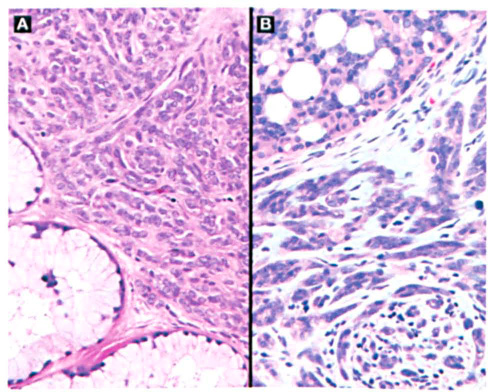
A mixture of patterns—often described as “the eye of the storm” or “swirling”—is characteristic. The neoplastic cells are often arranged in single-file infiltration at the periphery of the tumor (figure 2). Small tubules or ducts can be seen in the columns or nests of the tumor cells. The cells are small, uniformly bland, and polygonal to round and are arranged in a syncytium with indistinct cell borders (figure 3). There is usually ample cytoplasm surrounding round to oval nuclei with open, vesicular nuclear chromatin distribution. Small nucleoli may be seen. This proliferation is set within a gray-blue stroma that is often hyalinized (figure 2). Mitoses are exceedingly uncommon, and when they are present are difficult to find. The tumor cells show a biphasic immunophenotype with both epithelial and myoepithelial markers.
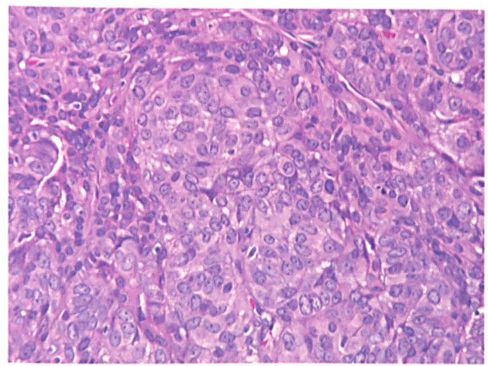
The nuclei of a PLGA are cytologically bland, with open vesicular nuclear chromatin and small nucleoli. Note the syncytial architecture.
PLGAs must be distinguished from pleomorphic adenomas and adenoid cystic carcinomas. Pleomorphic adenomas (1) are nodular, (2) lack perineural invasion, (3) tend to contain plasmacytoid cells and a myxoidchondroid matrix, and (4) usually exhibit strong immunoreactivity to glial fibrillary acidic protein. In adenoid cystic carcinomas, (1) a cribriform pattern is usually identified, (2) there is no swirling pattern, (3) nuclei are peg- or carrot-shaped and angular with nuclear hyperchromasia, (4) glycosaminoglycan is seen in the background, and (5) there is usually an elevated mitotic index (>3/10 high-power-fields).