
Abstract

Rhabdomyolysis is a potentially life-threatening disease process of skeletal muscle breakdown that leads to the release of intracellular contents into the circulation, as well as depletion of intravascular water and calcium through “third spacing.” It has various causes, including a direct toxic effect, physical or electrical trauma, extremes in exercise or temperatures, prolonged immobilization or compression, certain medications, infections, and electrolyte abnormalities. Symptoms include muscle pain, weakness, dark urine, swelling, fever, and altered mental status. A creatine kinase (CK) level greater than 5 times the upper limit of normal is considered diagnostic for this disease. 1 Rhabdomyolysis most commonly occurs in the legs and lower back; cases involving the head and neck are rare. 2
We present a case of rhabdomyolysis of the masticator space in a 38-year-old man. The patient had been running outdoors during the winter in the Midwest region of the United States when he suddenly developed severe right facial and bilateral calf pain, weakness, and numbness. He was found unconscious on a sidewalk. Emergency medical responders reported that the duration of his immobility and the specific position of his body when he was first discovered were unknown.
Physical examination revealed severe swelling and tenderness of the right side of the patient's face. Laboratory studies showed a CK level of 300 IU/L and a creatinine level of 5 mg/dl. The diagnosis of rhabdomyolysis was established by magnetic resonance imaging (MRI) of the head/neck and the lower extremities at presentation and by MRI and computed tomography (CT) on outpatient follow-up (figure).
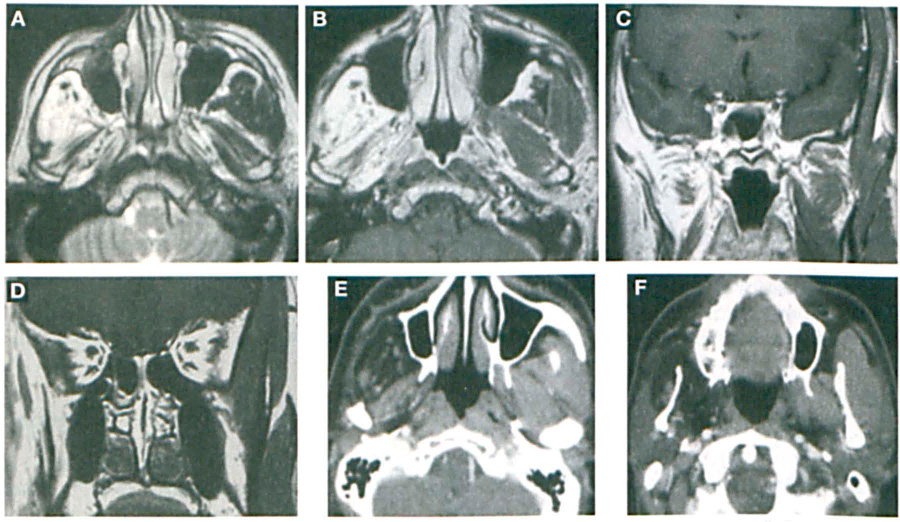
MRI and CT examinations show the abnormal masticator space on the right that is
consistent with rhabdomyolysis. During the acute stage, axial T1-weighted MRI
(
Rhabdomyolysis has traditionally been a clinical diagnosis, with imaging findings being a supporting factor.1,2 Head and neck rhabdomyolysis can mimic other head and neck conditions such as an inflammatory process, blunt trauma, a neoplasm, and autoimmunity disorders, among others. Imaging—particularly MRI because of its high degree of sensitivity—provides good support in the appropriate clinical context. 3
To the best of our knowledge, only 3 other cases of head and neck rhabdomyolysis evaluated by imaging have been reported in the literature.2,4,5 In each case, the disease process was precipitated by ingested toxins. In 2 of these cases,2,4 the affected muscles were on the side of the body that the patient had been lying on for a prolonged period of time. In all 3 cases, the initial diagnosis was not rhabdomyolysis; the unusual clinical presentations in these cases led the clinicians to think first of an abscess, streptococcal skin infection, cerebral edema, and stroke. Imaging was performed either to rule out these entities or to evaluate further the persistence of facial swelling despite treatment. A combination of imaging and the clinical picture led to the recognition of rhabdomyolysis.
Our case is unusual in that it was caused by a combination of strenuous exercise performed in a cold temperature. Extreme exercise relative to the level of an individual's physical conditioning may deplete cellular energy supplies, leading to damage of cellular membranes with continued activity. Cold exposure may play a role via peripheral vasoconstriction. 1
Our patient was found lying on a sidewalk; he might have been lying in the prone position with the right side of his head in contact with the cold pavement. Two of the previously described patients2,4 were found in a similar circumstance. Prolonged pressure on gravity-dependent body parts can induce ischemia; upon relief of such pressure, rhabdomyolysis can occur as a result of a reperfusion injury of the compressed area, leading to the release of necrotic material into the circulation. 1
Our patient's CK level was not especially elevated. It is important, however, to note that CK levels begin to rise 2 to 12 hours after an injury and they peak 24 to 72 hours afterward. 1 Our patient might have been in the early stages of rhabdomyolysis when he was examined, and thus his CK level would not have been noteworthy. This case illustrates the importance of using imaging in the appropriate clinical setting, especially with a creatinine level of 5 mg/dl.
We have used this opportunity to show our patient's imaging findings in the acute stage and later during follow-up. In 1 previously reported case of rhabdomyolysis of the masticator space, 5 follow-up imaging revealed resolution with apparently no significant sequelae. Our patient apparently experienced a more severe case of rhabdomyolysis that resulted in significant sequelae manifested by atrophy involving the muscles of the entire masticator space.