
Abstract
Sarcoidosis is a systemic inflammatory disease that can affect virtually every organ system, leading to a wide variety of clinical manifestations. Central nervous system involvement producing neurologic symptoms can occur in patients with sarcoidosis, yet rarely are these symptoms the initial manifestations of the disease. Here we present the case of a 38-year-old man who presented with a history of chronic facial pain, blurred vision, increased lacrimation, and periodontal abscesses. Physical examination revealed no evidence of infection or neoplasm. Magnetic resonance imaging revealed space-occupying lesions in Meckel cave bilaterally, with soft-tissue density extending into the left sphenoid and posterior ethmoid sinuses. Endoscopic biopsy of sinus mucosa demonstrated the presence of noncaseating granulomas and the absence of organisms, findings suggestive of neurosarcoidosis. The diagnosis was further supported by chest radiography, which demonstrated bilateral hilar adenopathy. The patient was treated with corticosteroids, and his facial pain improved markedly. In this article we discuss neurosarcoidosis and its manifestations, diagnosis, and clinical course.
Introduction
Sarcoidosis is a granulomatous disease that can affect any organ system but typically involves the lungs, skin, lymph nodes, and anterior uvea. Although the underlying cause of sarcoidosis is unclear,1–3 several studies have implicated genetic predisposition, depressed systemic cellular immunity, and specific pathogens (mycobacteria and Propionobacterium acnes in particular) in its pathophysiology.3–5
The pathognomonic finding in sarcoidosis on biopsy of affected tissue is the presence of noncaseating epithelioid granulomas, which represent masses of activated macrophages, epithelial cells, monocytes, and fibroblasts. These granulomas can form in any organ system, including the central nervous system (CNS) and peripheral nervous system, and therefore can manifest as focal neurologic findings. CNS involvement most commonly affects the skull base and cranial nerves, with symptoms reflecting the structures involved. 5 Imaging results are generally nonspecific but may show ill-defined mass lesions. Therefore, neurosarcoidosis should be considered in the differential diagnosis for patients presenting with chronic facial pain with abnormalities on imaging.
Case Report
A 38-year-old man presented to our clinic with a 2-year history of headache, severe left facial pain and, more recently, left midfacial paresthesia. Dental evaluations over the previous 2 years had led to the extraction of 3 maxillary teeth (teeth 14-16) because of periapical abscess formation. These sites had healed adequately, but the extractions had provided no benefit in terms of his facial pain. Previously obtained computed tomography (CT) of his head had demonstrated mild mucosal thickening in the maxillary sinuses but had identified no masses or other discrete abnormalities.
Our physical examination revealed no masses, mucosal abnormalities, or fistulae at the left maxillary alveolus extraction sites. Moderate tenderness and soft-tissue thickening without any discrete mass were observed over the medial portion of the left infraorbital rim. Nasal endoscopy showed mildly edematous mucosa with no masses or pathologic secretions. The remainder of the patient's exam was unremarkable.
Given the chronicity of the patient's symptoms and refractoriness to dental intervention, magnetic resonance imaging (MRI) was obtained to assess for a CNS lesion. Precontrast (figure 1) and postcontrast (figure 2) axial and coronal T1-weighted images demonstrated enhancing T1 signal intensity relative to adjacent white matter partially filling Meckel cave bilaterally. Enhancing soft tissue was also seen in the left sphenoid sinus and posterior ethmoid cells. Neurosurgical consultation was obtained, and concern was raised for a neoplasm.
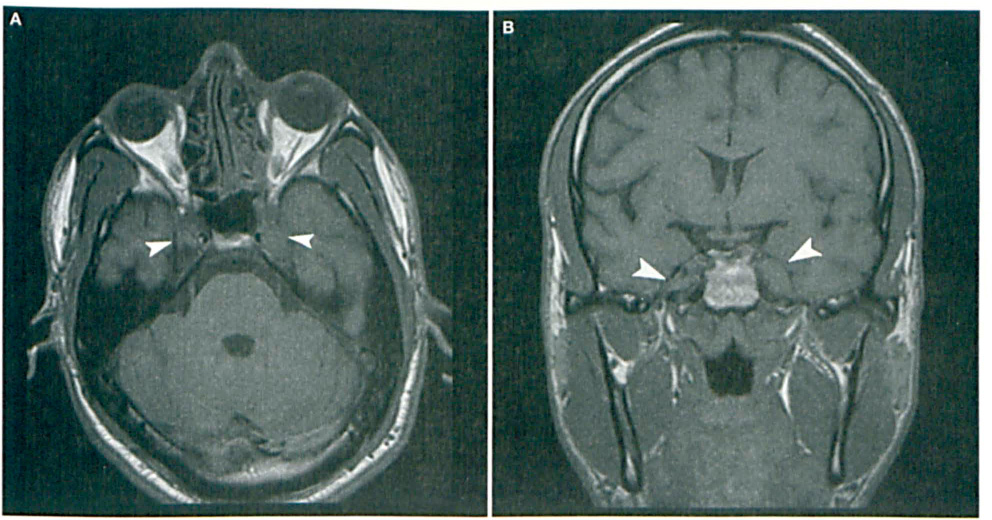
Precontrast axial (
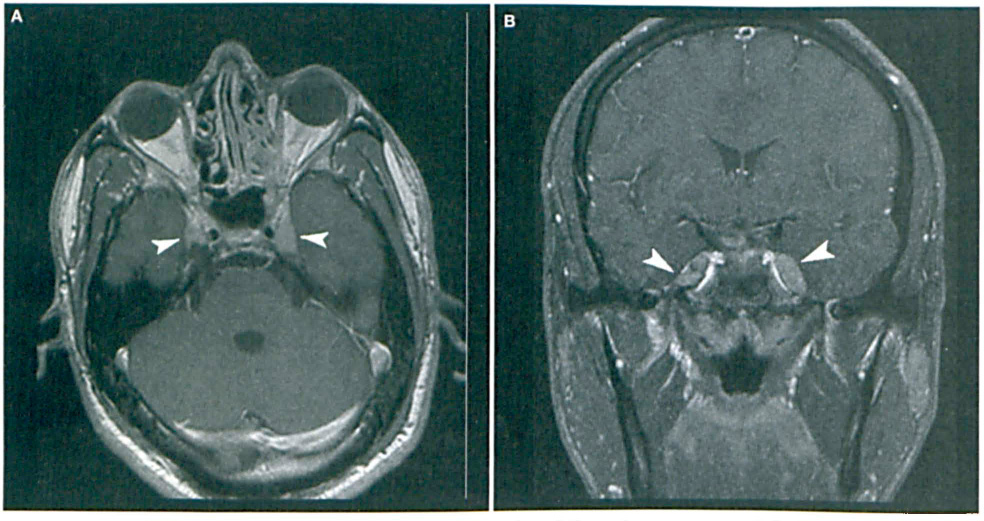
Postcontrast axial (
To obtain tissue for histopathologic examination, the left posterior ethmoid cells and sphenoid sinus were opened endoscopically. Intraoperatively, the ethmoid sinus mucosa was thickened and pale, but no obvious masses were identified. Frozen sections of mucosa revealed non-necrotizing granulomas, with Giemsa, periodic acid-Schiff (PAS), light green PAS, and Zeihl-Neesen stains all negative for organisms. As these findings were highly suspicious for sarcoidosis, chest radiography was obtained, which demonstrated bilateral hilar adenopathy, confirming the diagnosis.
The patient was started on oral corticosteroid therapy, which gave him modest relief from his facial pain, and referred to the neurology service for long-term management.
Discussion
Neurologic involvement occurs in as many as 10% of patients with sarcoidosis.6–8 The most common sequela is cranial neuropathy, but epileptic seizures, meningitis, mass lesions, spinal cord disease, psychiatric manifestations, movement disorders, and peripheral nerve disease have also been reported. 9 Neurologic complications of sarcoidosis are believed to arise as the result of a disruption of the leptomeningeal blood-brain barrier, which allows the granulomatous process to follow the Virchow-Robin perivascular space and enter the brain parenchyma. 10 Typically, neurologic findings are seen in patients with previously diagnosed sarcoidosis, although infrequently they may be initial findings and thus can present a diagnostic challenge, as with the patient presented here.
Gadolinium-enhanced MRI has become the most useful imaging study in evaluating the patient with possible neurosarcoidosis and is superior to contrast-enhanced CT in delineating neurologic involvement. 11 MRI findings in neurosarcoidosis include nonenhancing periventricular white matter lesions, meningeal enhancement, hydrocephalus, cranial nerve involvement, enhancing brain parenchymal lesions, dural mass lesions, and spinal cord involvement.12–15 In most cases these abnormalities are nonspecific and thus can mimic other CNS disorders such as multiple sclerosis, benign and malignant neoplasms (e.g., meningioma, astrocytoma, or metastatic lesions), or infectious lesions as seen with tuberculosis or bacterial or fungal lesions.
The coalescence of multiple granulomas in the brain parenchyma can produce space-occupying lesions, most commonly in the optic chiasm, floor of the third ventricle, and pituitary stalk, but can occur anywhere in the CNS. In the current case, the patient's facial pain arose from granuloma formation in Meckel cave with involvement of the trigeminal ganglia.
In addition to imaging, other nonspecific CSF findings, such as pleocytosis, increased opening pressure, low glucose levels, elevated lysozyme and β2-microglobulin, elevated helper-suppressor T-lymphocyte ratio, CD4:CD8 ratio >5, and elevated angiotensin-converting enzyme levels, have been reported in neurosarcoidosis.14,16–20 The utility of these tests in confirming the diagnosis is limited by their lack of specificity, as both infectious processes and malignancies can present with similar CSF findings. However, they may be helpful in particularly puzzling cases in which MRI or other studies do not provide definitive information. In the majority of cases, the definitive diagnosis of neurosarcoidosis requires direct histologic evidence of noncaseating granulomas, which prompted our patient's endoscopic biopsy.
When neurosarcoidosis is suspected in an individual without a previous diagnosis of sarcoidosis, investigations for evidence of systemic disease should be initiated. The most useful of these is chest radiography, as 31 to 80% of cases of neurosarcoidosis will demonstrate abnormalities. 21 The typical radiographic finding is bilateral hilar adenopathy, as was found in our patient, but pulmonary infiltrates and pulmonary fibrosis have also been observed. High-definition CT of the chest is also useful in evaluating pulmonary disease as it is more sensitive in detecting hilar and mediastinal adenopathy, as well as pulmonary infiltrates. Other tests for systemic sarcoidosis, such as whole body gallium staining, blind organ tissue biopsy, and blood tests for angiotensin-converting enzyme levels, are also used but have low specificity.16,22,23
The treatment of neurosarcoidosis is high-dose corticosteroids, although no rigorous studies evaluating the efficacy of different treatment regimens exist. Typically (and in this case), patients with neurosarcoidosis and cranial neuropathy are treated with 1.0 mg/kg/day of prednisone and often require prolonged therapy. 5 In addition, 20 mg/kg/day of IV methylprednisolone for 3 days or infliximab therapy has also been demonstrated to provide relief to patients with severe symptoms.
A variety of alternate immunosuppressive therapies have been employed with some success, including azathioprine, cyclophosphamide, methotrexate, myco-phenolate mofetil, cyclosporine, and chlorambucil. 24 The efficacy of these agents, however, has not been studied in appropriate placebo-controlled trials.
In conclusion, neurosarcoidosis should be included in the differential diagnosis of any patient presenting with chronic facial pain and nonspecific imaging findings. As this case illustrates, MRI may be useful in the diagnostic evaluation of cranial neuropathies to exclude other possibilities, but definitive diagnosis of neurosarcoidosis requires direct histologic evidence so that appropriate treatment may be initiated.