
Abstract
Dermal inclusion cysts are benign masses that arise as the result of the entrapment of ectodermal components during embryogenesis. Their presenting symptoms are a direct result of the mass effect of the growingcyst. We describe the case of a 23-month-old girl who presented with a single, large dermal inclusion cyst in the external auditory canal. Our review of the literature revealed that only 2 other cases of a dermal inclusion cyst in this location have been previously reported.
Introduction
Dermal inclusion cysts—also called dermoid cysts or simply dermoids— are rare, benign, developmental lesions. While they present during a wide range of ages, they are believed to be of congenital origin. 1 The contents of these cysts include hair, squamous epithelium, and glandular tissue. Presenting symptoms are primarily attributable to the mass effect. A cyst might rupture and cause infection and inflammation. 2
Dermal inclusion cysts are primarily found in the gonads; they are uncommon in the head and neck region. When they do occur in the head and neck, more than 80% are located in the orbit, oral cavity, or nasal cavity; they are extremely rare in the external auditory canal.2,3 We report a new case of dermal inclusion cyst of the external auditory canal. To the best of our knowledge, only 2 other cases have been previously reported in the literature.3,4
Case Report
A previously healthy 23-month-old girl was referred to us for evaluation of a new lesion that had arisen within the right external auditory canal. She was asymptomatic, and she had no history of otitis media, otitis externa, or trauma to her ears. On physical examination, she appeared to be well, and her speech and hearing were normal for her age.
Right otoscopy detected a soft-tissue swelling in the external auditory canal. The swelling did not allow even the smallest speculum to pass far enough to visualize the tympanic membrane. On inspection of the left ear, the canal and tympanic membrane were normal. Audiometry demonstrated a sound-field awareness of 15 dB. There was negative pressure on the left and a flat tympanogram on the right.
Computed tomography (CT) demonstrated a soft-tissue density within the ear canal; the mass had displaced the tympanic membrane medially (figure 1). There was no evidence of bony erosion, and the remainder of the middle ear, inner ear, and mastoid was developmentally normal. Radiographic examination indicated a clear middle ear cavity and an intact ossicular chain.
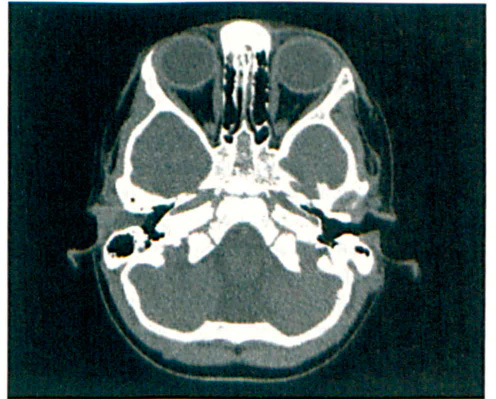
Preoperative axial CT of the temporal bone shows the soft-tissue mass within the right external auditory canal.
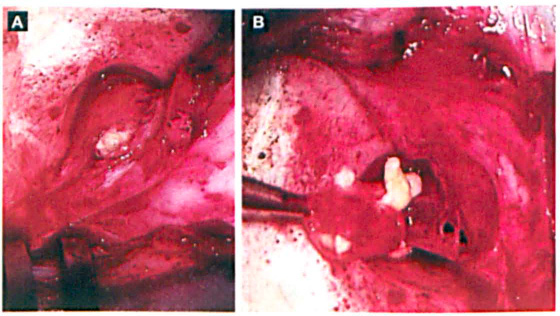
With the patient under general anesthesia, the mass was surgically removed via a postauricular approach. It was located in the subcutaneous tissue of the posterior external auditory canal (figure 2). There was a clear dissection plane between the mass and the epithelial lining of the canal. The cyst was encapsulated and filled with squamous debris and hair. Since the cyst extended medial to the annulus, the middle ear was explored. Except for a 1- to 2-mm extension from the lateral membranous canal medial to the inferior annulus, the middle ear was free of disease.
The entire cyst was removed with preservation of the overlying canal skin. The external canal was packed with ofloxacin-soaked Gelfoam, and the patient experienced an uneventful postoperative course.
On gross examination, the excised mass measured 1.3 × 0.4 × 0.2 cm. The final histologic report identified it as a dermal inclusion cyst.
On follow-up, the external auditory canal was widely patent and well epithelialized, and the family reported that the child was more responsive to noises on her right side.
Discussion
Dermal inclusion cysts are derived from ectodermic elements entrapped during the midline fusion of the first and second branchial arches. This stage of embryogenesis occurs between the third and fourth week of intrauterine life. While epidermoid and dermoid cysts have similar origins, they differ in their degree of differentiation; epidermoids contain only squamous epithelium, while dermoids contain hair and glandular tissue in addition to squamous epithelium.
Some epidermoid cysts are congenital, while others arise as a result of a traumatic insult the leads to implantation of epithelial tissue.1–3 Epidermoid cysts are also extremely rare in the external auditory canal. 5 Dermoid cysts most commonly present in the second and third decades of life, which is slightly earlier than the typical onset of epidermoids. 2
The differential diagnosis of a mass lesion within the external auditory canal can be quite extensive. The list includes various benign and malignant tumors, cholesteatoma, epidermal inclusion cyst, and first branchial cleft cyst. CT, magnetic resonance imaging, and fine-needle aspiration biopsy can aid in the diagnosis of a dermal inclusion cyst.1,2
On imaging, both epidermoids and dermoids are unilocular lesions. While dermal inclusion cysts exhibit variable imaging characteristics, they are generally associated with a thicker cystic wall that can calcify. Sebaceous lipid material produces a signal intensity similar to that of fat, resulting in a fat-fluid level within the cyst. 2 However, a definitive diagnosis is possible only after excision and histologic examination.
Dermoid cysts of the head and neck account for approximately 6.9% of all dermoids found in the body.1,3 In a 2009 report, Al-Khateeb et al reviewed 488 head and neck cysts and found that dermoid cysts accounted for 22%. 1 The periorbital area was the most common location of these cysts (52% of cases); in descending order, the next most common locations were the neck, scalp, and the periauricular, nasal, and buccal areas. These findings are consistent with similar studies of the prevalence of different cysts.
Of the 2 previously reported cases of dermal inclusion cyst of the external auditory canal, 1 involved multiple cysts 3 and the other involved a solitary cyst. 4 Boo et al described multiple cysts in an 11 -year-old girl. 3 Her course was similar to the one in our patient in that her only notable symptom was unilateral aural fullness. In that case, a second encapsulated mass was discovered in the operating room and removed. She, too, had an uncomplicated postoperative follow-up without any signs of recurrence. The other case was reported in Russian by Khudainazarov et al in 1981. 4
The standard treatment for a dermal inclusion cyst is surgical excision. The indications for surgery include a pathologic diagnosis, removal of an occlusion, prevention of infection and inflammation, and correction of a cosmetic defect. 3 As is the case with all types of cysts, if the capsule is not completely removed, the risk of recurrence is increased. In view of the slow growth rate of dermoids, treatment is not urgent, but it should take place while the cyst is asymptomatic.