
Abstract
An 11-year-old girl presented with hoarseness and voice fatigue. These symptoms had adversely affected her participation as a singer and dancer in a school performance group. Her history included excision of a 9-cm neck teratoma shortly after birth. Strobovideolaryngoscopy revealed right vocal fold paralysis. The patient was administered 1 mg of intravenous cefazolin and then treated with an autologous fat injection into the right vocal fold.
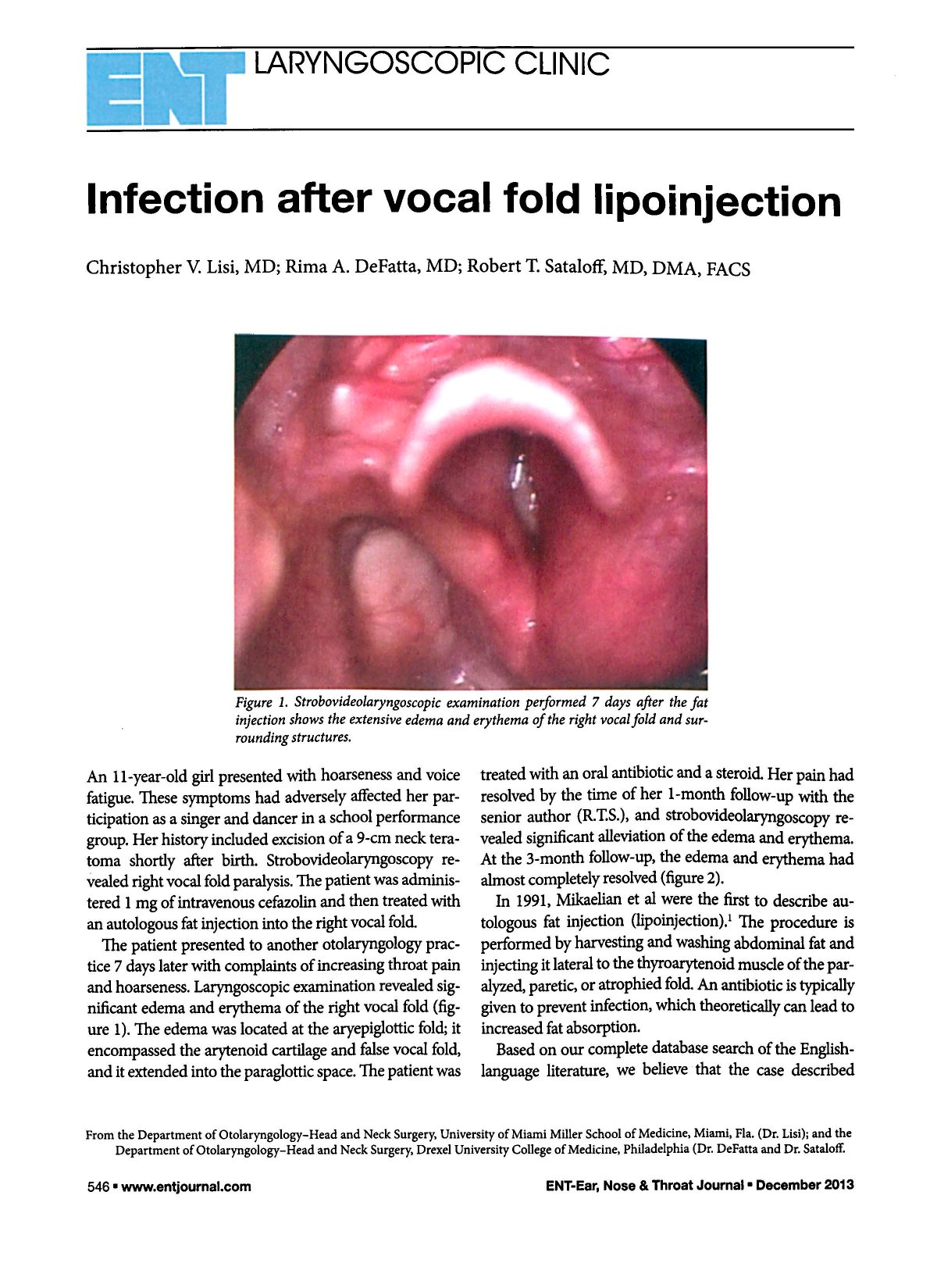
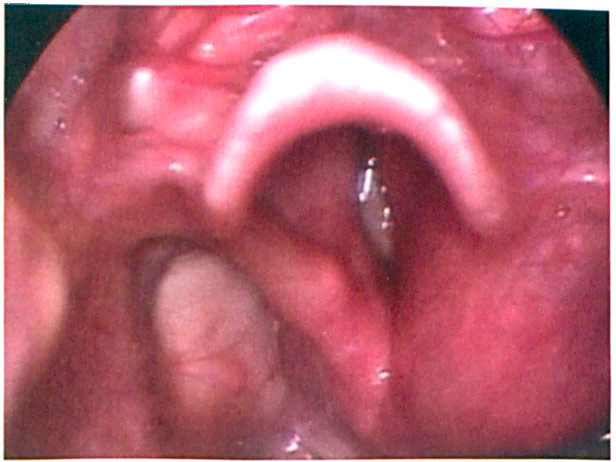
The patient presented to another otolaryngology practice 7 days later with complaints of increasing throat pain and hoarseness. Laryngoscopic examination revealed significant edema and erythema of the right vocal fold (figure 1). The edema was located at the aryepiglottic fold; it encompassed the arytenoid cartilage and false vocal fold, and it extended into the paraglottic space. The patient was treated with an oral antibiotic and a steroid. Her pain had resolved by the time of her 1-month follow-up with the senior author (R.T.S.), and strobovideolaryngoscopy revealed significant alleviation of the edema and erythema. At the 3-month follow-up, the edema and erythema had almost completely resolved (figure 2).
Strobovideolaryngoscopic examination performed 7 days after the fat injection shows the extensive edema and erythema of the right vocal fold and surrounding structures.
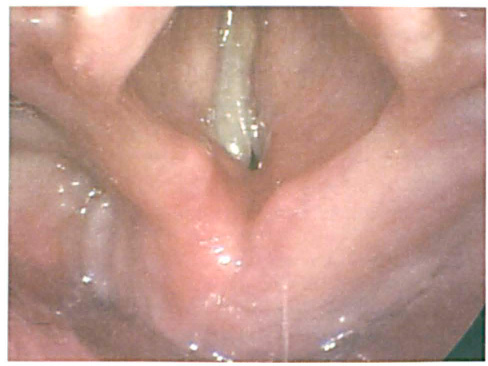
Three months after the fat injection, the edema and erythema are almost completely resolved.
In 1991, Mikaelian et al were the first to describe autologous fat injection (lipoinjection). 1 The procedure is performed by harvesting and washing abdominal fat and injecting it lateral to the thyroarytenoid muscle of the paralyzed, paretic, or atrophied fold. An antibiotic is typically given to prevent infection, which theoretically can lead to increased fat absorption.
Based on our complete database search of the English-language literature, we believe that the case described herein represents the first reported instance of a vocal fold infection after an autologous fat injection for vocal fold paralysis. Indeed, Laccourreye et al specifically noted the absence of infection as a complication in their review of 80 patients treated with this procedure. 2
The infection in our patient occurred despite our use of proper sterile technique when harvesting the abdominal fat, as well as the administration of a prophylactic antibiotic prior to the injection. We attribute the infection of this area to inoculation of the vocal fold with the normal flora of the aerodigestive tract. Our patient was recovering nicely and had no untoward effects from the infection at the time of her 3-month follow up. However, the effect of this complication on fat survival and vocal fold position will require long-term follow-up.