
Abstract
Chronic subdural hematoma as a complication of lumbar drain placement for the management of iatrogenic cerebrospinal fluid (CSF) leak has not been previously documented in the literature. We describe such a case in a 69-year-old man who presented with right nasal obstruction secondary to an inverted papilloma involving the paranasal sinuses. The patient underwent endoscopic sinus surgery, which included a medial maxillectomy. Surgery was complicated by a small CSF leak, which was repaired intraoperatively. Five days later, the patient experienced CSF rhinorrhea, and a lumbar drain was inserted. He developed overdrainage symptoms but was well when he was discharged. However, 22 days later he returned with right hemiparesis. Computed tomography of the brain showed a left frontoparietal subdural hematoma with a mass effect. The neurosurgical team performed an emergency drainage procedure, and the patient experienced a complete neurologic recovery. We discuss the pitfalls of lumbar drainage, the possible pathophysiology of overdrainage, and the lessons learned from this case.
Introduction
As more anterior skull base surgeries are being performed endoscopically by otorhinolaryngologists, we are faced with a greater likelihood of encountering neurosurgical complications. Cerebrospinal fluid (CSF) rhinorrhea at the anterior skull base is a rare complication of such endoscopic endeavors. A lumbar drain is sometimes placed perioperatively as a shunt to reduce the leak.
Chronic subdural hematoma as a complication of lumbar drainage for the management of iatrogenic CSF leak has not been previously documented in the literature. We describe what we believe is the first such case, and we discuss the pitfalls of lumbar drainage in cases of iatrogenic CSF leak, the possible pathophysiology of overdrainage, and the lessons learned from this case.
Case Report
A 69-year-old man presented to our ENT clinic with a 6-month history of right nasal obstruction. He was otherwise asymptomatic. Endoscopic nasal examination detected the presence of polyps filling the right nasal cavity; the lesions were papillomatous in appearance. Biopsy analysis confirmed inverted papilloma of the nose. Computed tomography (CT) of the paranasal sinuses demonstrated involvement of the right maxillary sinus, ostiomeatal complex, frontal recess, and ethmoid air cells.
The patient underwent endoscopic sinus surgery, which included a medial maxillectomy. Surgery was complicated by a small CSF leak (<2 mm in diameter) over the cribriform plate. The leak was repaired intraoperatively with a free mucoperiosteal graft (underlay technique) from the inferior turbinate. With help from the anesthesiologist, confirmation of the seal was verified with the Valsalva maneuver at the conclusion of the operation. The patients right nostril was packed with Merocel.
The patient was ventilated overnight and extubated the next day. He was prescribed a laxative, intravenous ceftriaxone, a cough suppressant, and strict bed rest. The Merocel was removed on postoperative day 3. The patient was well until postoperative day 5, when he developed CSF rhinorrhea during straining. He was then referred to the neurosurgery unit for insertion of a lumbar drain, which was placed to drain at bed level.
Three days later, the patient complained of worsening occipital headaches when he sat up to eat; the headaches abated when he would lie down. Otherwise, he remained afebrile and exhibited no clinical evidence of CSF rhinorrhea. Daily biochemical and culture studies of the lumbar CSF ruled out any infection. The 24-hour lumbar drain chart showed the following consecutive readings:
86 ml during the remaining 12 hours of day 1;
241 ml on day 2;
315 ml on day 3; and
111 ml during the first 12 hours of day 4.
At that point, the drain was removed. Endoscopic examination of the anterior skull base confirmed an absence of CSF leakage. The patient was discharged home in good condition on postoperative day 9.
Twenty-two days later, the patient was readmitted for evaluation of weakness in the right upper and lower limbs; the weakness had become worse over the previous few days (grade 3). He was alert and conscious, and no spontaneous CSF leak had occurred.
An urgent CT of the brain showed a left frontoparietal subdural hematoma with a mass effect (figure). The patients bleeding profile and platelet count were normal. The next day, the neurosurgical team placed the patient under general anesthesia and then inserted a drain through a left parietal burr hole. Intraoperatively, 10 ml of fluid was drained. No active bleeding was seen.
The patients recovery was uneventful, his muscle power improved, and he was discharged 3 days later. Findings on a repeat CT of the brain 2 months later were normal. On review at 5 months postoperatively, the patient had regained full muscle power, and his right nasal cavity remained free of disease.
Discussion
Inverted papillomas are relatively uncommon nasal tumors. Some long-standing lesions have been known to undergo malignant transformation. Endoscopic medial maxillectomy and sinus surgery are increasingly being used for complete removal of these lesions. As is the case with all endoscopic procedures, a possible surgical complication of such procedures is a breach of the skull base resulting in CSF leakage; this is especially risky if important landmarks are obscured or altered by a nasal mass. In our case, the iatrogenic CSF leak was small, and closure of the leak was verified intraoperatively.
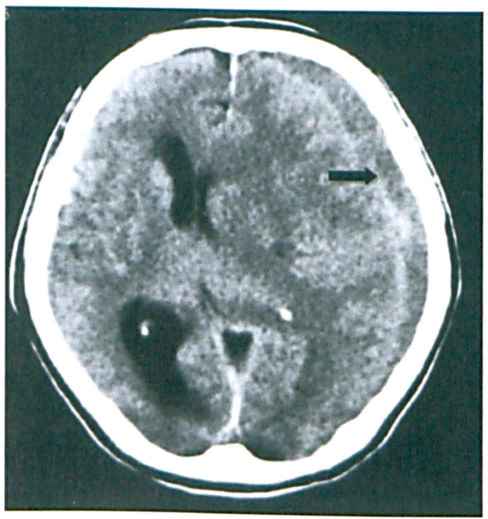
Axial CT shows the mixed subdural iso- and hyperdense collection in the left frontoparietal area (arrow). At its widest (1.5 cm) point, the mass has caused compression of the lateral and third ventricles, with a midline shift to the right. The right lateral ventricle is mildly dilated
In our experience, lumbar drainage has not been used routinely. In this case, the lumbar drain was inserted only after the CSF leak recurred on postoperative day 5. It is difficult to say in retrospect if the free graft might have been displaced during removal of the intranasal packing or if there was a temporary rise in intracranial pressure during extubation.
Subdural hematoma following a lumbar drain insertion is exceptionally rare. While cases of subdural hematoma after spinal anesthesia and ventriculoperitoneal shunt placement have been described in the literature, our case was different in that the patient experienced a delayed leak accompanied by chronic subdural hematoma, even though he was well when first discharged. Menon et al reported a case in which a patient had collapsed as a result of an acute subdural hematoma following lumbar drainage for an iatrogenic CSF leak that had occurred during transsphenoid surgery; despite the drainage, the patient remained physically disabled. 1
Risk factors for subdural hematoma after lumbar drainage are overdrainage, older age, and tension pneumocephalus. Overdrainage reduces the CSF volume and intraventricular pressure. This can lead to dural separation from the brain and stretching of the bridging vein, which increases the risk of rupture. Headache is the most common symptom of intracranial hypotension, and it is believed to arise as a result of the descent of the brain after a loss of CSF buoyancy. 2 This places traction on pain-sensitive structures such as the cerebral veins and arteries.3,4 This would explain the postural nature of orthostatic headaches and the symptomatic relief that occurs upon lying down.
Overdrainage also creates more space for the accumulation of subdural fluid. 5 Therefore, it is important to ensure that the drain is clamped while the patient is sitting up, because sitting up is the most common cause of overdrainage. Our patient displayed the classic symptoms of overdrainage, as he complained of headaches that became worse when he sat up to eat and then experienced relief when he became supine. Although his symptoms abated after a few hours, his total CSF volume on the final full day of drainage was 315 ml. On retrospective analysis, a high index of suspicion might have alerted us to the possibility of an intracranial pathology, and an urgent CT of the brain might have led to an earlier diagnosis of the subdural hematoma.
Typically, the head end of the bed is elevated 30° and the receiving chamber of the lumbar drain is positioned at the level of the tragus. The importance of clamping the drain cannot be overemphasized, even in a busy ward setting in a tertiary care hospital. With nursing assistance, a drain should be clamped to prevent accidental overdrainage before the patient sits up or otherwise moves around. When the patient lies down again, the nurse should readjust the level of the drip and reopen the drain. Proper attention must also be given to the positioning of the drain catheter, especially when the patient moves, and to making sure that it does not fall out unnoticed for a prolonged duration.
The risk of subdural hematoma is higher in an aging atrophic brain, so older patients should receive special attention. A tear in the dura can lead to tension pneumocephalus, 6 but it is unlikely that this occurred in our patient because his leak was small and repaired immediately.
The routine use of a lumbar drain in the repair of a CSF leak remains debatable. Some surgeons routinely use them, 7 while others have achieved a high rate of success without them.8,9 Some surgeons recommend them more selectively, reserving them for patients with a high-volume or long-standing CSF leak. 10 Even though we do not routinely use a lumbar drain, it proved to be useful in our patient, although it did cause a rare late complication.
In conclusion, there is always a risk of CSF leak in skull base endoscopic surgeries, more so if important landmarks are obscured or altered by the tumor. Lumbar drainage has a role in the management of CSF leaks. It is important that proper positioning and timely clamping of the drain not be taken lightly. While subdural hematoma following the placement of a lumbar drain is exceptionally rare, surgeons must be aware of the possibility. The diagnosis of this potentially catastrophic condition would benefit from a high index of suspicion and a low threshold for investigation.