
Abstract
Nasal fractures are usually diagnosed by clinical examination, with or without the support of imaging studies. While plain-film radiography lacks sensitivity and specificity for diagnosing nasal fractures, and computed tomography (CT) is not always practical or cost-effective, ultrasonography (US) may be useful in this regard. The criteria by which adult nasal fractures are reliably identified on US must be clear. We conducted a preliminary prospective, controlled, observational study to define the appearance of nasal fractures on US. We used US to image 12 patients with a clinical or radiologic (CT or x-ray) diagnosis of nasal fracture. All patients presented within 2 weeks of their injury. For comparison purposes, we also obtained US images from 12 control subjects who had no history of nasal trauma or surgery. We found that we could confidently diagnose nasal fractures on lateral-view US on the basis of a disruption of bone continuity and/or displacement of fracture segments. However, our findings were not as consistent with dorsal-view US, and we do not believe it is adequate for diagnosis. We conclude that lateral US can be used to detect nasal fractures in adults, but further studies are needed to assess its sensitivity, specificity, cost-effectiveness, and practicality.
Introduction
Historically, the gold standard for diagnosing nasal fractures has been the clinical examination. 1 Physical findings typically include nasal deformity, mobility, crepitus, and edema; swelling often precludes a definitive diagnosis until it abates. Imaging modalities such as computed tomography (CT) and plain-film radiography have been used to support the diagnosis of nasal fracture. However, studies have shown that plain films are neither sensitive nor specific for adults in this regard, and while CT is good for imaging complex fractures, it is expensive and often impractical in the setting of an isolated nasal fracture. 2
Ultrasonography (US) is a safe and easy imaging tool that is usually used in the head and neck region to identify pathologic changes in soft tissue. It has long been shown to be useful in the diagnosis of fractures of the larger bones, such as the skull, clavicle, and ribs. US has been used to identify fractures of the facial bones, including the zygomatic arch, orbit, and frontal sinus. 3
At the time of this study, the literature contained few studies of the use of US in diagnosing nasal fractures. Thiede et al 4 reported that US was equal to conventional radiography, and Hong et al 1 reported that US can be used as a primary diagnostic technique in children. More recent studies have further advocated the use of US in diagnosing nasal fractures.5–8
In this article, we describe our study of the usefulness of US in diagnosing nasal fracture, and we present the criteria by which a diagnosis can be confidently established.
Patients and Methods
From January to May 2007, we performed a prospective, nonrandomized, controlled, observational study of the use of US in patients with a diagnosis of nasal fracture. Our exclusion criteria were a previous nasal fracture or sinonasal surgery, including sinus surgery and septorhinoplasty, and age less than 16 years (for the purposes of this study, potential subjects aged 16 or 17 years were considered to be adults).
A total of 24 subjects were enrolled— 12 patients with nasal fracture and 12 normal controls. The fracture group was made up of 10 men and 2 women, aged 17 to 71 years (mean: 34.8); there were 10 whites and 2 blacks (table 1). The control group included 6 men and 6 women, aged 23 to 73 years (mean: 39.4); there were 7 whites, 2 blacks, 2 Asians, and 1 American Indian (table 2).
Summary of Cases
Number of days since injury.
Key: CT = computed tomography; US = ultrasonography; Pos = positive; Neg = negative, N/A = not applicable; MVA = motor vehicle accident.
Demographic Data for the Control Group
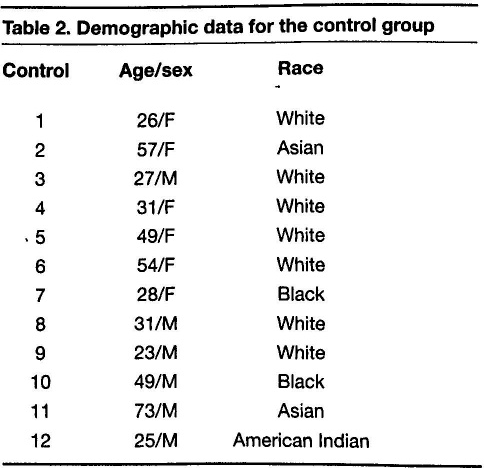
The patients in the fracture group had been diagnosed on the basis of a clinical examination, CT (figure 1), and/ or plain film radiography, and all had presented within 10 days of their injury. The choice of imaging was made at the discretion of the treating Emergency Department physician. After evaluation by the Emergency Department staff, we obtained US images with a 40-mm flat 5–12 mHz probe (Accuvix XQ; Samsung Medison USA; Cypress, Calif.).
Coronal (
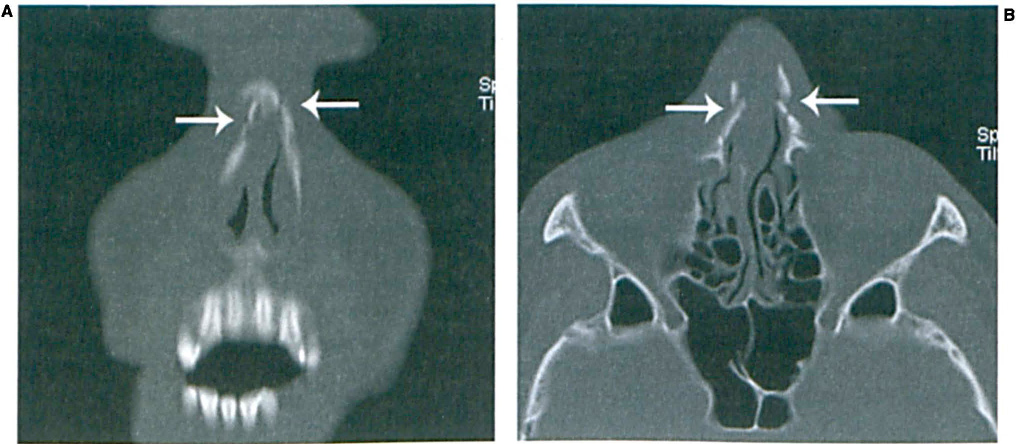
US images were obtained in the right and left lateral views and in the dorsal view (figure 2). These images were later reviewed and discussed by a team of 4 otolaryngologists, who determined whether nasal bones were either fractured (positive) or not fractured (negative). Controls were imaged in the same manner with the same equipment.
US is obtained in the lateral (
The study protocol was approved by the Institutional Review Board at the University of North Carolina.
Results
Ten of the 12 patients were evaluated for nasal fracture by facial CT at the time of their presentation to the Emergency Department (table 1). Of the 2 remaining patients, 1 (patient 6) was diagnosed on the basis of a clinical examination and plain film x-ray and the other (patient 11) underwent only a clinical examination.
The team of 4 otolaryngologists had access to the official radiology reports for all CTs and x-rays. Two members of the team had participated in the collection of the US images. The review process involved an open discussion of the fracture and control US images, and decisions as to whether an image was sufficient to diagnose a fracture were reached by consensus.
We were able to confidently differentiate between fracture and nonfracture on US images obtained in the lateral view (figure 3). From this exercise, we were able to determine that certain criteria are sufficient to diagnose a nasal fracture in the lateral view. These criteria are disruption of bone continuity and/or displacement of fracture segments. We were unable to confidently differentiate between fractures and nonfractures on US images in the dorsal view (figure 4).
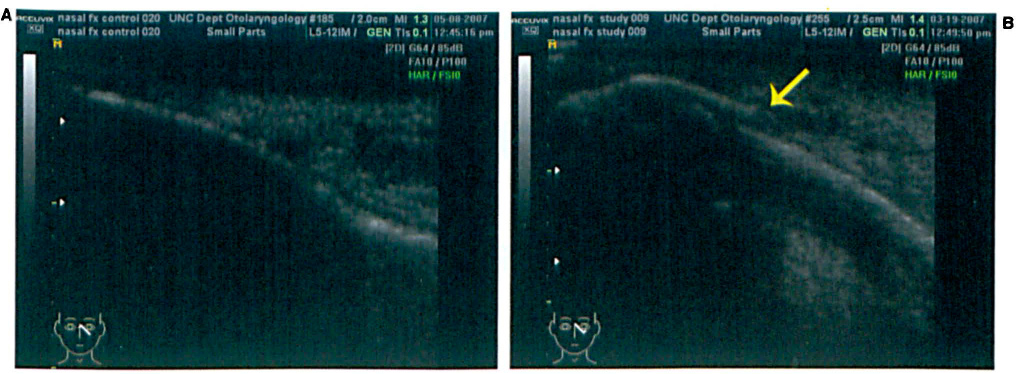
Lateral-view US demonstrates a normal left side in a control subject
(
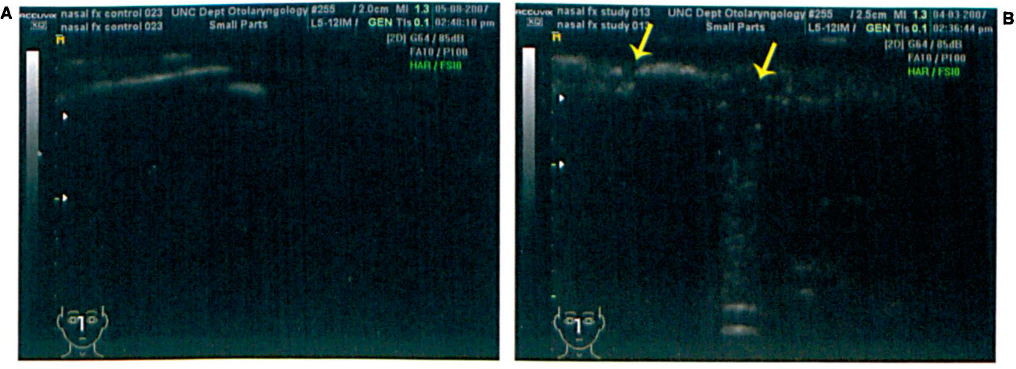
Dorsal-View US Shows a Control Subject (
Discussion
Most nasal fracture patients present with significant edema, which makes the physical examination difficult for the provider and painful for the patient. In many cases, patients are asked to return in 1 week to allow time for swelling to subside. Nasal fractures more than 2 weeks old can be technically difficult to reduce and painful for the patient, thus requiring operative intervention.
Contemporary radiographs have been shown to have low sensitivity and specificity for nasal fracture.1,2 Although patients with signs of multiple and complex facial injuries may warrant CT, isolated nasal fractures do not. A reliable, efficient, and inexpensive imaging study that does not expose the patient to radiation would be very useful in diagnosing nasal fractures. Moreover, such imaging could prove to be very useful in the evaluation of postreduction results.
The purpose of our study was to identify specific criteria that could be used to diagnose adult nasal fractures on US, as such guidance has been lacking. Without such criteria, one cannot be certain of the diagnosis. Based on our observations, we concluded that in order to diagnose a nasal fracture by lateral US, the practitioner must see a disruption of bone continuity and/or displacement of fracture segments. This conclusion was arrived at by comparing the US images of normal controls with those of patients with fractures that had been diagnosed by clinical examination, CT, and/or plain-film radiography.
In view of the small number of participants in our study, strong statistical differences between the fracture and control groups could not be calculated. Our goal was to conduct a preliminary study to establish which criteria are useful to measure outcomes in future studies.
Our patients and controls did not experience any discomfort from the US gel or from the pressure exerted by the probe. Examinations were performed in less than 5 minutes. While the accuracy of a US examination is dependent on the skill of the operator, in our experience this technique can be learned very easily. The images can be interpreted by a care provider in real time or they can be reviewed later to provide a diagnosis.
In our study, the fracture locations were obvious in the vast majority of cases, and the panel of 4 otolaryngologists had no difficulty reaching a consensus. None of the control images showed any disruption of bony continuity or displacement. Only 1 patient (patient 8) had a fracture that could be seen on CT but not on US; however, that particular reading might have actually represented a nasal suture line that then led to a false-positive result.
We did find it difficult to identify clear differences between the fracture patients and control subjects when assessing the dorsal-view images. Both groups showed interruptions in bony continuity or displaced nasal segments, which likely represented anatomic suture lines (figure 4). Thiede et al demonstrated that dorsal-view plain films were superior to dorsal-view US images, which is consistent with our findings. 4 On the other hand, they also found that lateral-view US was superior to lateral-view x-rays.
In 2007, Hong et al demonstrated that US could be used as the primary diagnostic technique in evaluating nasal and septal fractures in children. 1 Children have a higher proportion of cartilage to bone in the nasal skeleton, which makes radiologic assessment easier than it is in adults.
Since the original presentation of our study at The Triological Society's Southern Section Meeting in 2008, other studies have used criteria similar to ours in defining nasal fractures by US. These studies have demonstrated sensitivities and specificities of greater than 90% in diagnosing nasal fractures with US.5–8 Lou et al outlined an algorithm that includes ultrasonography in the workup of isolated nasal fractures. 7 Furthermore, recent studies have shown US to be useful in assessing postreduction nasal contour intraoperatively,9,10 similar to its use in reducing zygomatic complex fractures. 11
This study demonstrates that ultrasonography, particularly in the lateral view, can be useful in identifying fractures based on disruption of bone continuity and/or displacement of fracture segments. Ultrasound should be considered in the algorithm for assessment and treatment of nasal fractures.