
Abstract

A 42-year-old man was referred to us with a 6-month history of dysphagia and regurgitation. He reported a 38-pound weight loss, and serum prealbumin indicated protein malnutrition at 17 mg/dl. He had a complex surgical history at an outside hospital, including anterior cervical discectomy and fusion (ACDF) in 2006 complicated by intraoperative esophageal perforation. Subsequently, multiple surgical attempts at repair were made. Recovery was prolonged by the patient's refusal to remain NPO.
A barium swallow was obtained (figure 1), which revealed a proximal diverticulum that did not appear like a typical Zenker diverticulum. The patient was taken to the operating room for endoscopic diverticulotomy. Endoscopic examination in the OR revealed visible cervical hardware on the anterior surface of the vertebral bodies in the pouch (figure 2). The procedure was aborted.
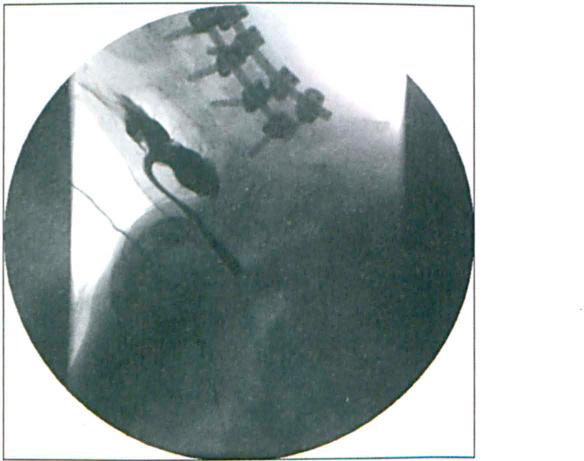
Gastrografin esophagogram reveals the large pharyngoesophageal fistula. The large “septum” in this iatrogenic diverticulum made it amenable to endoscopic treatment.

An endoscopic view of the proximal diverticulum shows food remnants, separated from the esophagus by a large “septum.”
The patient was taken back to the OR with the neurosurgical team for removal of the exposed hardware and closure of the anticipated defect. Examination of the hardware after removal showed food particles embedded within the cage. Tissue quality was noted to be extremely poor, and a three-layered closure was performed and bolstered by a sternocleidomastoid muscle flap. Despite this, postoperative wound breakdown occurred and the fistula was surgically externalized. The pharyngocutaneous fistula subsequently healed by secondary intention with daily wound packing.
Fistula closure was confirmed with barium swallow, leaving the patient with the iatrogenic pharyngoesophageal diverticulum. He subsequently underwent CO2 laser endoscopic diverticulotomy with good results. On follow-up evaluation he was gaining weight steadily and tolerating oral intake without any symptoms of dysphagia.
A pharyngoesophageal perforation is a rare but serious complication of ACDF surgery. The incidence ranges from 0.2% to 1%, most commonly in the early postoperative period, but it can present as far out as several years postoperatively. Most perforations are thought to result from esophageal retraction, direct injury during manipulation, hardware failure, or movement of cervical vertebral bodies during hyper-extension. Mortality increases with treatment delay. Imaging studies, such as computed tomography of the neck, should be performed to confirm the diagnosis. Esophagography (with water-soluble contrast agent) and occasionally flexible endoscopy can also help locate perforations and fistulas.
Treatment for pharyngoesophageal perforations after ACDF should be tailored for each patient. Well-contained leaks with small perforations and no signs of septicemia may respond to conservative treatment. For delayed or larger pharyngoesophageal perforations, surgical closure with reinforcement using muscle is desired. Dysphagia is often a significant presenting symptom, and malnourishment should be recognized if present. Optimization of patient's nutrition status is important to allow wound healing, and occasionally surgical repair may be delayed to allow enteral feedings to restore adequate nutritional status.
Other factors associated with poor wound healing (such as diabetes or poor vascular status) should be taken into account and will impact management strategy and patient counseling.
Once the perforation is healed, patients with expected persistent phyarngoesophageal diverticulum may benefit from endoscopic or open repair.