
Abstract

An 11-month-old infant boy presented to the otolaryngology service for evaluation of recurrent acute otitis media, persistent middle ear effusions, and reactive airway disease. He was a former 33-week premature infant with a cardiac history of patent foramen ovale and had been intubated for 1 week after birth. Over the subsequent 11 months, he had intermittent wheezing thought to be due to reactive airway disease, which was treated with nebulizers.
Given the patient's history, a bronchoscopy was planned to be performed while he was under anesthesia for myringotomy tube placement. The bronchoscopy revealed a tracheal bronchus. (figure 1). No significant collapse or retained secretions were present. Postoperatively, a computed tomography (CT) scan of his chest showed the right upper lobe bronchus arising from the distal trachea, above the carina (figure 2). The patient has been asymptomatic for more than 2 years since his diagnosis.
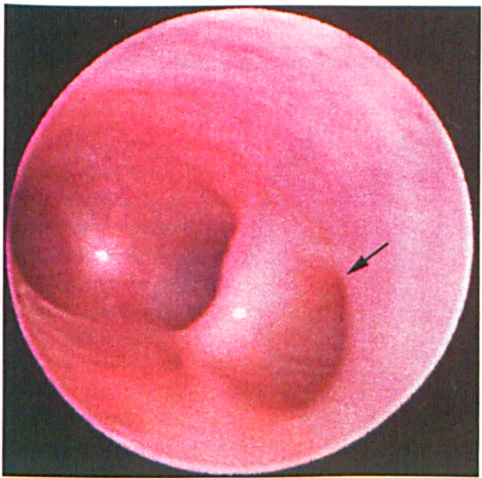
Intraoperative Photograph Shows the Right Upper Bronchus Arising from the Trachea Proximal to the Carina (Arrow).
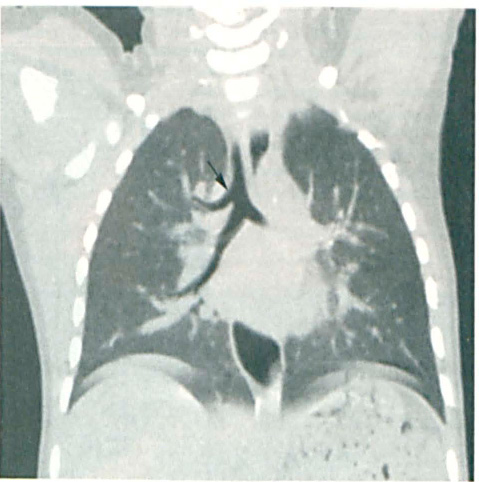
Coronal CT Scan Demonstrates the Tracheal Bronchus Arising from the Distal Trachea (Arrow).
A tracheal bronchus is an aberrant right upper lobe bronchus arising from the distal trachea proximal to the carina. Alternatively, it has been referred to as bronchus suis, or pig bronchus, as a tracheal bronchus is a normal finding in swine and other ruminants. The incidence has been reported as 0.001 to 2%, depending on the means of diagnosis (bronchoscopic, radiographic, or cadaveric).1,2 Therefore, most otolaryngologists will have diagnosed a patient with this anomaly at some time in their careers.
There is an association between tracheal bronchus and other congenital malformations of the ribs and vertebrae, as well as a higher association in children with Down syndrome. 3 In most cases, the diagnosis is made incidentally during routine bronchoscopy performed for other issues. While most patients are asymptomatic, it is important to remember that this anomaly may be associated with significant morbidity, and possibly mortality. 4
The possibility of a tracheal bronchus should be entertained when a patient presents with recurrent right upper lobe pneumonia or right upper lobe collapse. The cause in these cases is thought to be retained secretions distal to the anomalous bronchus. Other presenting symptoms include stridor, respiratory distress, and symptoms indicative of foreign body aspiration or a thoracic mass. 3
A tracheal bronchus also may have important implications for airway management and lung isolation during general anesthesia for other thoracic procedures. 5 Ultimately, a right upper lobectomy may be required for management of recurrent pneumonia and atelectasis of the anomalous right upper lobe. Bronchoscopy and CT scan should be performed to confirm the diagnosis and ensure that no other airway anomaly or pulmonary pathology exists that requires treatment.
Because tracheal bronchus, while uncommon and usually asymptomatic, may be associated with significant morbidity and possibly mortality, clinicians should keep this anomaly in mind when evaluating a patient with recurrent symptoms localized to the right upper lobe region. Persistence of recurrent or chronic airway disease may warrant diagnostic bronchoscopy to confirm the diagnosis.