Abstract

Undifferentiated carcinoma (also known as anaplastic carcinoma) of the thyroid gland is a highly aggressive malignant neoplasm composed of undifferentiated cells that exhibit immunohistochemical or ultrastructural epithelial differentiation. Nearly all patients report a long history of thyroid gland disease, often goiter or Hashimoto thyroiditis. In most cases, there is a transformation from a papillary (80%) or follicular carcinoma into undifferentiated carcinoma. Radiation exposure is reported in about 10% of patients.
While accounting for only 2% of all thyroid gland malignancies, undifferentiated carcinoma accounts for >60% of thyroid cancer mortality. The majority of patients are elderly, with a slight female predilection. Patients present with a rapidly enlarging, firm-hard neck mass, usually involving a single lobe (60%). In addition, many patients also report hoarseness, vocal fold paralysis, and pain. Soft-tissue or adjacent organ (esophagus, trachea) extension by the tumor is common.
In spite of multimodality therapy, the prognosis is still grave, with >95% of patients dead from disease in <9 months. There is a worse prognosis for patients aged >60 years, male, with >5-cm tumors or extensive local disease. By definition, all tumors are pT4 and separated into groups IVA, IVB, and IVC based on extent of local and metastatic disease. The tumors are fleshy to firm, usually replacing the thyroid gland parenchyma, with an infiltrative and irregular border. They nearly always show extrathyroid gland extension. The tumors are large, with a mean size of 6 cm.
Histologically, undifferentiated thyroid carcinomas show a variety of patterns, from sheet-like, storiform, fascicular, angiomatoid, and meningothelial to solid, exhibiting extensive lymph-vascular invasion. There is usually extensive coagulative-type necrosis, hemorrhage, and degeneration. Colloid is absent, but entrapped follicles can mimic colloid production.
The tumor cells are poorly differentiated, yielding a polygonal, pleomorphic, spindle, giant, epithelioid, or squamoid appearance. Tumor giant cells and osteoclastic giant cells are seen (figure 1). Mitoses are easily identified, are increased, and include atypical forms. Several histologic variants are recognized and include spindle cell, pleomorphic giant cell, squamoid, osteoclastic, rhabdoid, and angiomatoid variants, among others.
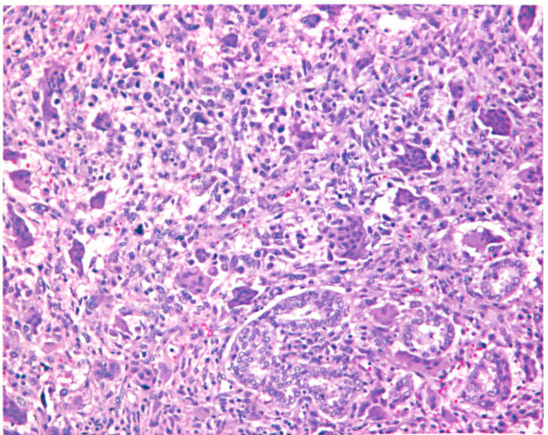
An undifferentiated carcinoma is present in association with a papillary carcinoma (lower right). Note the osteoclastic-type giant cells.
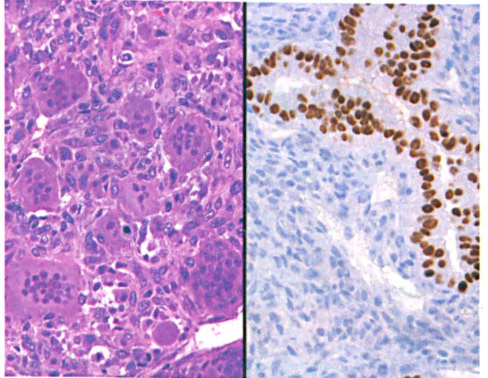
Because of the pleomorphic nature of the tumor, immunohistochemistry is frequently employed to confirm a diagnosis. Most tumors exhibit vimentin, keratin, CAM5.2, EMA, β-catenin, and p63 immunoreactivity, while usually negative with thyroglobulin and TTF-1 (figure 2); p53 and Ki-67 are usually strongly positive. The histologic differential diagnosis includes metastases to the thyroid gland (carcinoma, sarcoma, melanoma); primary sarcoma, lymphoma, and several primary thyroid gland malignancies (including medullary thyroid gland carcinoma); and Riedel thyroiditis.