
Abstract
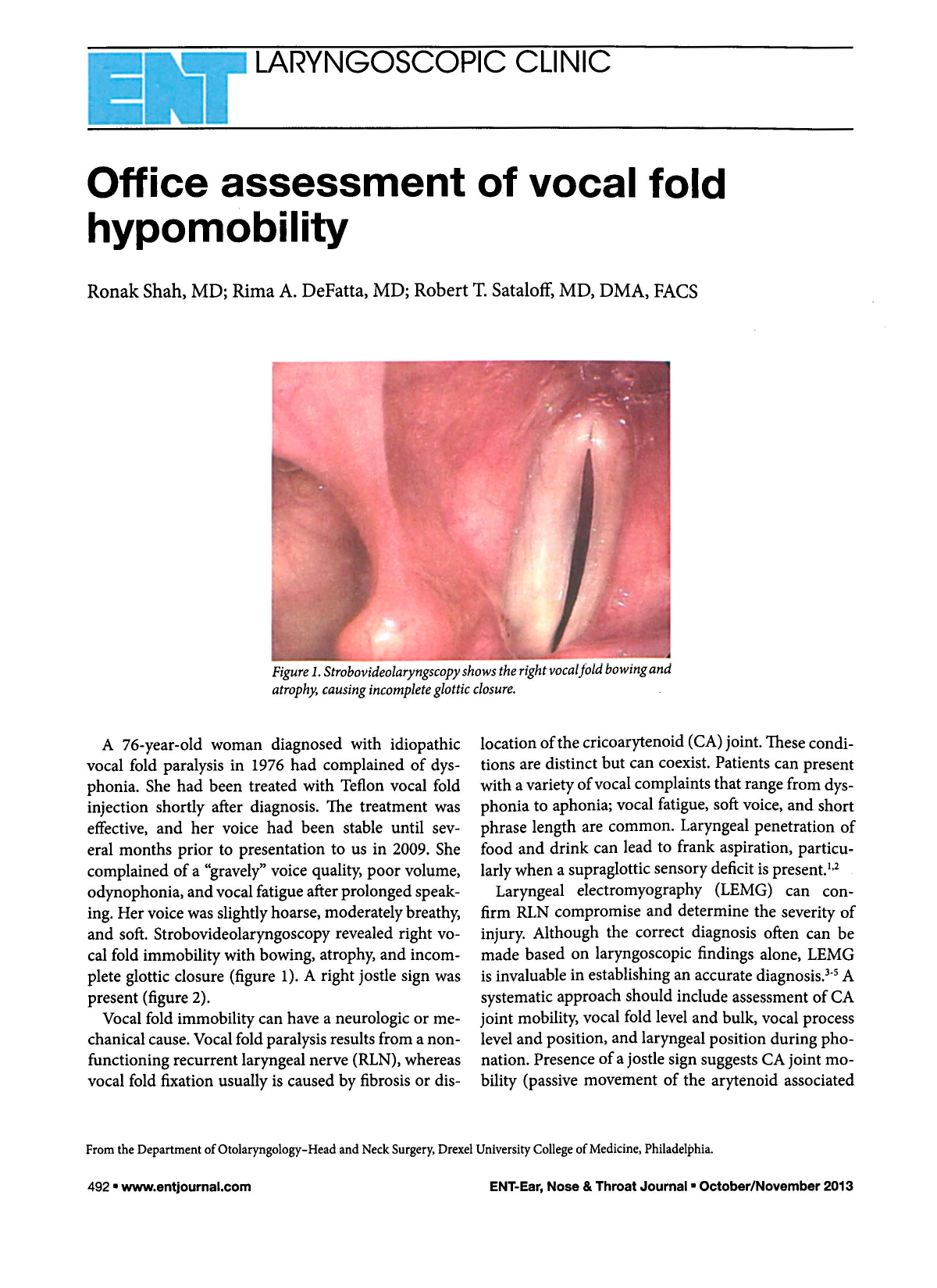

Strobovideolaryngscopy Shows the Right Vocal Fold Bowing and Atrophy, Causing Incomplete Glottic Closure.
A 76-year-old woman diagnosed with idiopathic vocal fold paralysis in 1976 had complained of dysphonia. She had been treated with Teflon vocal fold injection shortly after diagnosis. The treatment was effective, and her voice had been stable until several months prior to presentation to us in 2009. She complained of a “gravely” voice quality, poor volume, odynophonia, and vocal fatigue after prolonged speaking. Her voice was slightly hoarse, moderately breathy, and soft. Strobovideolaryngoscopy revealed right vocal fold immobility with bowing, atrophy, and incomplete glottic closure (figure 1). A right jostle sign was present (figure 2).
Vocal fold immobility can have a neurologic or mechanical cause. Vocal fold paralysis results from a nonfunctioning recurrent laryngeal nerve (RLN), whereas vocal fold fixation usually is caused by fibrosis or dis-location of the cricoarytenoid (CA) joint. These conditions are distinct but can coexist. Patients can present with a variety of vocal complaints that range from dysphonia to aphonia; vocal fatigue, soft voice, and short phrase length are common. Laryngeal penetration of food and drink can lead to frank aspiration, particularly when a supraglottic sensory deficit is present.1,2
Laryngeal electromyography (LEMG) can confirm RLN compromise and determine the severity of injury. Although the correct diagnosis often can be made based on laryngoscopic findings alone, LEMG is invaluable in establishing an accurate diagnosis.3–5 A systematic approach should include assessment of CA joint mobility, vocal fold level and bulk, vocal process level and position, and laryngeal position during phonation. Presence of a jostle sign suggests CA joint mobility (passive movement of the arytenoid associated with the paralyzed fold when contacted by the arytenoid of the normal fold during adduction).

The presence of a right jostle sign indicates passive movement of the arytenoid on the paralyzed side caused by contact with the normal arytenoid, which presses against it during adduction. It is seen most easily at the muscular process. This image also highlights laryngeal rotation toward the paralyzed side during phonation. Contraction of the normal side pulls the laryngeal framework to the left of the esophageal inlet, which is seen here posteriorly and to the right.
Vocal fold findings depend upon the location and extent of injury, as well as the degree of neural regeneration and synkinesis. Long-standing vocal fold paralysis without reinnervation usually leads to incomplete glottic closure, vocal fold atrophy and bowing, and decreased vocal process and vocal fold heights. However, partial neural regeneration is common and can prevent muscle atrophy and bowing by maintaining muscle tone.
Even though abductor-adductor fiber mismatch often leads to net vocal fold immobility, the preserved muscle tone sometimes permits glottic closure through compensation by the normal vocal fold. For this reason, early reinnervation procedures in cases with a poor prognosis may be beneficial when performed before the onset of muscle atrophy. 2