
Abstract
A 42-year-old man presented to our department with a worsening left-sided hearing loss. He had a history of a left-sided type III tympanoplasty and had undergone placement of a hydroxyapatite total ossicular replacement prosthesis (TORP) by an outside otolaryngologist 4 years earlier because of recurrent otitis media and hearing loss. He denied experiencing tinnitus, otalgia, otorrhea, vertigo, and imbalance. He also denied prior noise exposure or otologic trauma. He had no right-sided otologic symptoms. His medical history was significant for chronic hepatitis C and type II diabetes mellitus.
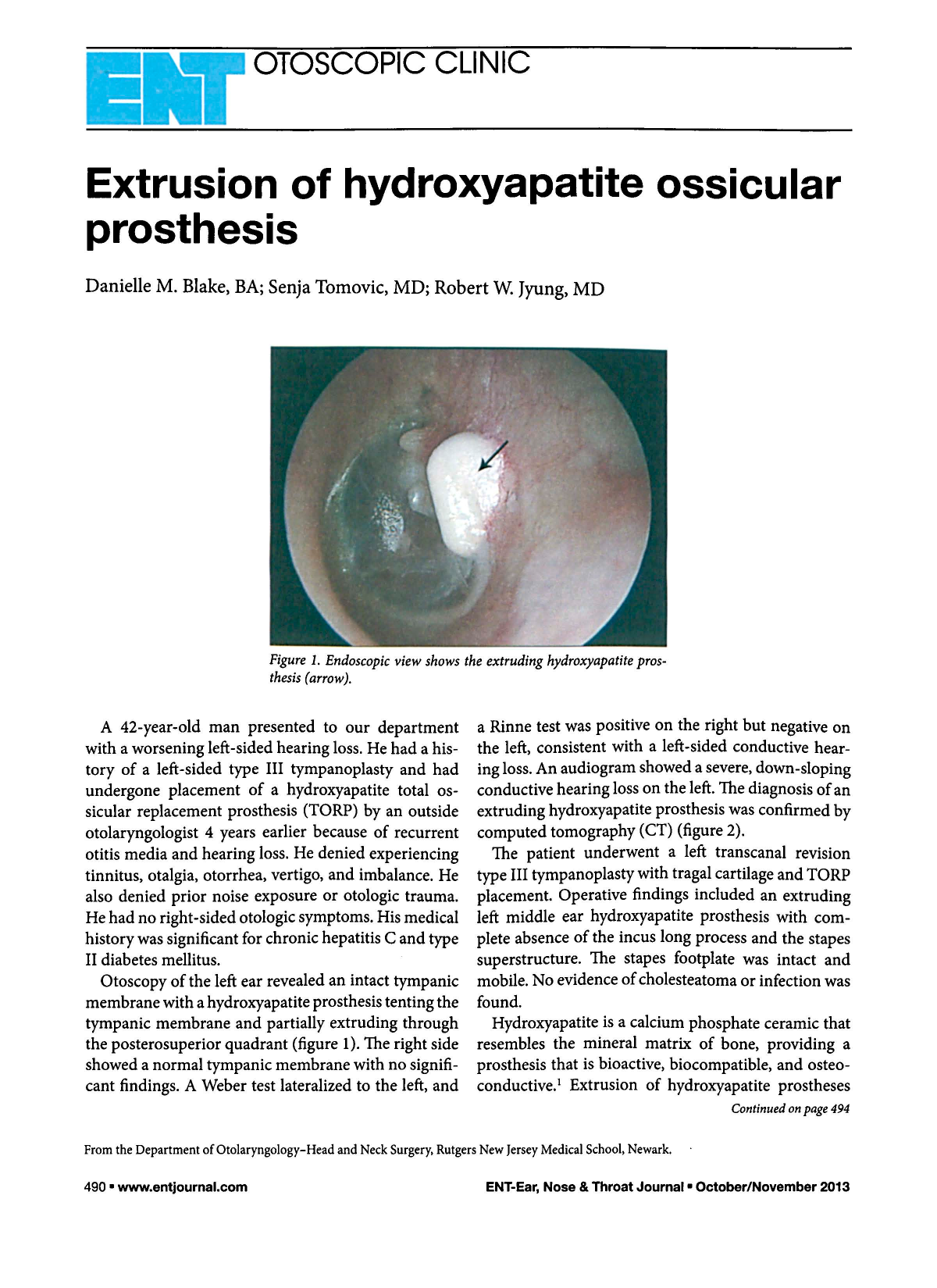
Otoscopy of the left ear revealed an intact tympanic membrane with a hydroxyapatite prosthesis tenting the tympanic membrane and partially extruding through the posterosuperior quadrant (figure 1). The right side showed a normal tympanic membrane with no significant findings. A Weber test lateralized to the left, and a Rinne test was positive on the right but negative on the left, consistent with a left-sided conductive hearing loss. An audiogram showed a severe, down-sloping conductive hearing loss on the left. The diagnosis of an extruding hydroxyapatite prosthesis was confirmed by computed tomography (CT) (figure 2).
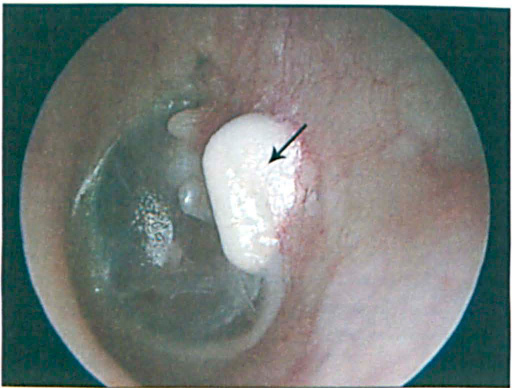
Endoscopic View Shows the Extruding Hydroxyapatite Prosthesis (Arrow).
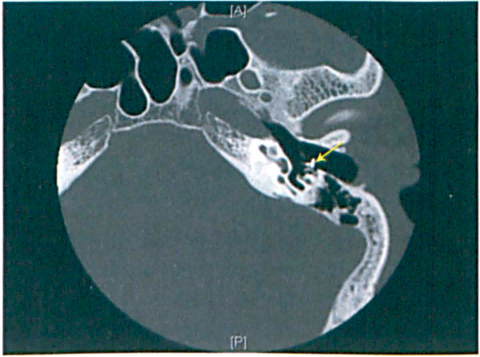
Axial CT Demonstrates the Extruding Prosthesis (Arrow).
The patient underwent a left transcanal revision type III tympanoplasty with tragal cartilage and TORP placement. Operative findings included an extruding left middle ear hydroxyapatite prosthesis with complete absence of the incus long process and the stapes superstructure. The stapes footplate was intact and mobile. No evidence of cholesteatoma or infection was found.
Hydroxyapatite is a calcium phosphate ceramic that resembles the mineral matrix of bone, providing a prosthesis that is bioactive, biocompatible, and osteoconductive. 1 Extrusion of hydroxyapatite prostheses is unfortunately a common complication of middle ear surgery. Reported extrusion rates range from 5 to 22%.2,3
Cartilage interposed between the prosthesis and tympanic membrane has been employed to decrease the chance of extrusion by providing a rigid autologous surface that prevents scarring of the tympanic membrane to the prosthesis. 4 The addition of interposed cartilage decreases the rate of extrusion to just 3 to 6%, allowing long-term retention and function of these prostheses. 3