
Abstract
We present 2 cases of advanced juvenile nasopharyngeal angiofibroma (JNA) to illustrate the advantages of endoscopic Coblation-assisted resection of intranasal extensions of these masses. Both patients—an 11-year-old boy and a 14-year-old boy—presented with a large, extensive mass (Radkowski stage IIIb and Fisch stage IVb in both cases). After embolization was performed on each patient, his JNA was partially ablated via an endoscopic approach with the Coblator II Surgery System with an EVac Xtra Plasma Wand in conjunction with an image-guided navigation system. Both patients experienced resolution of their nasal obstruction with removal of the intranasal extension of the tumor. Coblation allowed for a controlled debulking of the tumors with less blood loss and without the need for multiple instruments. To the best of our knowledge, our report is one of the first to describe image-guided endoscopic Coblation of advanced JNA tumors. Future studies in adequately sized populations are needed to determine the safety and effectiveness of Coblation-assisted endoscopic removal of both advanced and lower-stage JNAs.
Introduction
Juvenile nasopharyngeal angiofibroma (JNA) is a benign, locally aggressive tumor that primarily affects males in the second and third decades of life. Its highly vascular nature and friable structure leads to copious blood loss during resection, thus making it a tedious undertaking. Since Kamel's description of endoscopic transnasal resection of a JNA in 1996, 1 attention has been focused on improving minimally invasive endoscopic methods for removing these masses. Among the considerable benefits of the endoscopic approach are less intraoperative hemorrhage, a shorter postoperative recovery, and fewer cosmetic defects.2,3
Conservative endoscopic surgical procedures require hemostasis for adequate visualization. When such procedures are combined with embolization of tumor-feeding vessels, the incidence of intraoperative hemorrhage is significantly reduced. 4 However, tumor debulking of a JNA can still be hindered by frequent and copious bleeding, and thus this procedure has traditionally required more operative time and the need for additional surgical instruments.
Among the various methods of primary transnasal resection of advanced-stage JNAs that have been described in the literature are the harmonic scalpel, laser, microdebrider, and cold-knife instrumentation.3,5 To the best of our knowledge, there are no previously published reports of plasma-mediated radiofrequency-based ablation (Coblation; ArthroCare Corp.; Sunnyvale, Calif.) as an alternative in this situation.
It is our belief that endoscopic Coblation-assisted resection combined with preoperative embolization and image-guidance navigation may be a highly effective method of endoscopic surgery. We present 2 cases of JNA to emphasize the advantages of Coblation-assisted endoscopic surgery.
Case Reports
With Institutional Review Board approval, we retrospectively analyzed the operative management of 2 patients who had been diagnosed with JNA in 2009. We reviewed their history and clinical course to document intraoperative complications, operative times, transfusion requirements, and surgical outcomes (table). Following embolization of tumor-feeding vessels, both patients underwent definitive treatment with the use of the Coblator II Surgery System (ArthroCare) equipped with an EvacXtra Plasma Wand and facilitated by image-guided navigation.
Table. Case summaries
Packed red blood cells.
Patient 1
An 11-year-old boy was brought to our clinic with a 3- to 4-year history of nasal obstruction and recurrent acute sinusitis. Endoscopic examination detected a nearly complete obstruction of both nasal cavities (figure 1, A). Diagnostic imaging identified a large JNA (Radkowski 6 stage IIIb and Fisch 7 stage IVb) that extended into the nasal cavities, sphenoid sinus, right maxillary sinus, clivus, pterygoid fossa, anterior cranial fossa, and right middle cranial fossa abutting the temporal lobe (figure 1, B).
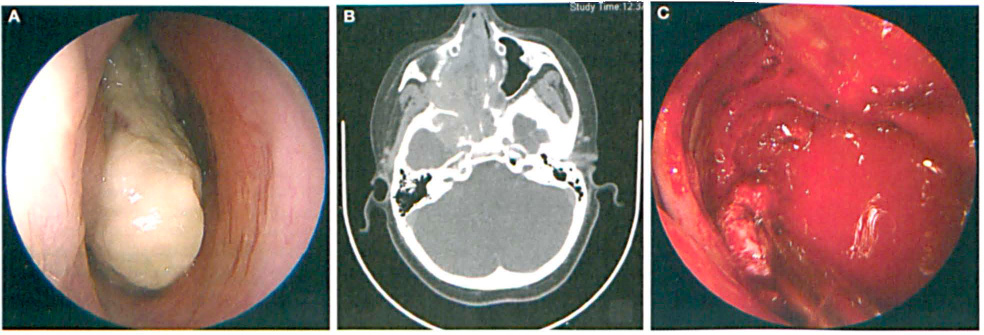
Patient 1. A: Preoperative image shows the JNA in the 11-year-old boy. B: CT shows the large, extensive JNA. C: The intraoperative hemorrhage is seen during resection with the microdebrider.
Prior to his scheduled excision, the patient twice presented to the emergency department for episodes of epistaxis, which resolved spontaneously in both cases. When he began to exhibit increased lethargy and a poor nocturnal oxygen saturation level, his surgery was rescheduled for an earlier date.
Despite embolization, intralesional hemorrhaging interrupted the first attempt at resection with Stryker 5 (Stryker; Kalamazoo, Mich.) and Medtronic M4 (Medtronic; Minneapolis) microdebriders (figure 1, C), and the resection was limited to the nasal cavity and surrounding structures. A second attempt performed 5 days later (again after embolization) resulted in further tumor removal with a microdebrider under image guidance, but the procedure was again complicated by considerable bleeding. Two units of packed red blood cells were transfused at time of the second embolization and 4 units intraoperatively.
After several frustrating failures to achieve hemostasis with bipolar suction cautery and nasal packing, we chose to finish the procedure with the Coblator II Surgery System. The switch to Coblation resulted in improved hemostasis and ease of tumor resection.
The patient recovered with minimal complications, and he was discharged home on postoperative day 5. He underwent postoperative radiation, and at follow-up 27 months after his initial procedure, he exhibited no evidence of tumor growth.
Patient 2
A 14-year-old boy presented to our clinic with a 2-year history of nasal obstruction. Imaging revealed the presence of a Radkowski stage IIIb and Fisch stage IVb JNA that extended into the nasal cavities, the paranasal sinuses, cavernous sinuses, left posterior orbit, and left middle cranial fossa (figure 2, A). For this case, we primarily used endoscopic Coblation with image-guided navigation to resect the tumor within both nasal cavities and the nasopharynx. While the JNA could not be removed in its entirety, palliative Coblation was successful in opening the nasal and nasopharyngeal airway and in improving the patient's breathing. This procedure was accomplished with much less blood loss (figure 2, B).
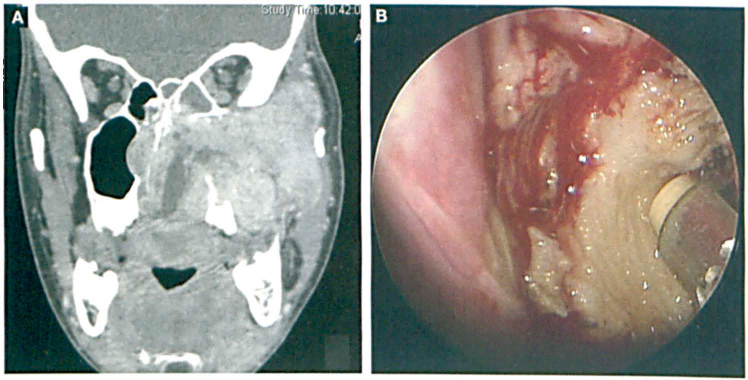
Patient 2. A: CT shows the large, extensive JNA in the 14-year-old boy. B: Much less blood loss is seen during Coblation-assisted debulking.
The patient recovered without complication. Right and left nasal packings were removed on the first and second postoperative days, respectively, and there was no recurrent epistaxis. The patient was discharged on postoperative day 3. On follow-up, his tumor continued to grow in several areas. Therefore, two subsequent palliative embolizations were performed to reduce the size of the mass, one at 12 months postoperatively and the other at 20 months. The first embolization resulted in stabilization of the size of the residual JNA. After the second embolization, magnetic resonance imaging demonstrated a small reduction in the size of the JNA.
Discussion
Both of our patients with advanced JNA achieved symptomatic relief of nasal cavity obstruction with either a combination of microdebrider and Coblation treatment (patient 1) or with Coblation alone (patient 2). Follow-up endoscopic examinations of the surrounding healthy tissue revealed no detectable injury.
Patient 1 required two visits to the operating room before a satisfactory resection of his nasal obstruction could be achieved. Embolization seemed to be less effective in this patient. After the failure of two attempts at embolization and resection with the microdebrider with bipolar and suction cautery, we turned to Coblation, and it was successful.
A noticeable decrease in blood loss occurred following the change of instruments in patient I's second surgery. He required a total of nine blood transfusions during the two operations and two more during embolization at an outside institution. Efforts to remove tumor extensions outside the nasal cavity and sinuses were limited because of the degree of intracranial invasion, and the patient required adjuvant radiation therapy for the remaining tumor in the inferior orbit, middle cranial fossa, and cavernous sinus. He reported no further episodes of epistaxis following the final Coblation procedure, and nasal airway patency was maintained on examination 2 months following surgery.
Patient 2 underwent a single debulking procedure with the Coblator, which removed all tumor tissue from both nasal cavities and the nasopharynx, and he experienced symptomatic relief. During his procedure, he was administered a single unit of blood as a precautionary step.
Multiple methods of treatment for advanced-stage JNA have been described, but surgical resection remains the preferred primary treatment. 8 In Coblation therapy, a single plasma wand is used for both tissue ablation and coagulation. Its use in diverse procedures such as tonsillectomy, adenoidectomy, and oral cancer resections carries the promise of potential applications in other areas of endoscopic surgery.9,10
In the case of our patient 1, the difficulties engendered by recurrent hemorrhage during the microdebrider procedures were intensified by the need to insert and remove multiple instruments in order to identify and control bleeding vessels. Yet, regardless of the choice of procedure, resection of JNAs is a tedious task. Nevertheless, Coblation may reduce the number of steps and instruments required to achieve hemostasis during resection.
Although using Coblation to debulk a tumor can be more time-consuming than using a microdebrider in the more fibrotic regions of a tumor, having the proper instrument in place for simultaneous hemostasis may shorten coagulation time and minimize visual-field obstruction secondary to bleeding. Coblation may also decrease injury to adjacent healthy tissue during debulking. Coblation's ability to spare surrounding tissue has been reported in removal of malignancies of the oral cavity, oropharynx, hypopharynx, and larynx. 10 The effectiveness of this method has been illustrated by minimal postoperative complications and rapid recovery.
The limitations of Coblation-assisted resection have not been formally evaluated in JNA resection. Tumor extension imposes considerable challenges with any method, and the risk of recurrence is high. Both of our patients underwent an incomplete resection because of concerns about potential bleeding from tumor-feeding vessels, the limitations of the nasal endoscopic approach, and the degree of intracranial extension. However, with Coblation we achieved our objective of symptomatic relief from nasal and nasopharyngeal obstruction without significant hemorrhage, injury to adjacent healthy tissue, or postoperative complications.
A small number of endoscopic surgeries for the removal of large tumors have been described. 11 The limitations of such procedures seem to be largely determined by the skill and experience of the surgeon. We anticipate that the same will be true for Coblation.
Finally, the usefulness of the Coblation device may be limited by its size and relative inflexibility, which could make it slightly more difficult to navigate along with the endoscopy. A future design modification of this instrument might improve its usefulness in this application. In addition, the use of Coblation for smaller, resectable JNA tumors likely has future merit and warrants investigation.
In summary, we conclude that image-guided endoscopic Coblation may be a safe and effective method of resecting intranasal portions of advanced JNAs. Other surgical methods are limited by the complex instrumentation required for adequate debulking and by concerns about frequent and copious intraoperative bleeding. The Coblator II Surgery System may limit the need for multiple instruments, and it may improve control of intraoperative hemorrhage in certain cases. Larger studies are needed to comprehensively evaluate the safety, effectiveness, and future applications of Coblation-assisted resection of JNAs.