
Abstract
Otogenic brain abscess and postauricular fistula are complications of chronic suppurative otitis media. We describe a rare case of bilateral chronic suppurative otitis media that caused a left temporal lobe abscess and a right mastoid fistula.
Introduction
Otogenic brain abscess is the second most common intracranial complication of middle ear infection; only meningitis is more prevalent. Reported mortality rates for otogenic brain abscess range widely—from 7 to 61%. 1 Approximately 50% of all brain abscesses in adults are of otogenic etiology. 2
In our review of the world literature, we could not find any previously published case of bilateral unsafe chronic suppurative otitis media (CSOM) with a left temporal lobe abscess and a right mastoid fistula. Therefore, we present a case of this unusual clinical presentation to instill awareness of its life-threatening potential.
Case report
A 57-year-old woman presented with a 3-day history of headache, giddiness, and slurred speech and a 2-day history of associated fever and drowsiness. She was admitted to the medical ward. Her history included a recurrent, foul-smelling, bilateral ear discharge with hearing impairment since childhood.
Clinical examination of the left ear confirmed the foul-smelling purulent discharge, along with a posterosuperior marginal tympanic membrane perforation, granulation material, and a cholesteatoma. Inspection of the right ear revealed a postauricular mastoid fistula with minimal keratin debris suggestive of a cholesteatoma (figure 1). No nystagmus or neck stiffness was noted. The patients left eye was covered with dense cataract. She was unable to walk because of decreasing consciousness.
The patient's Glasgow Coma Scale score was 13/15 (E4 V3 M6), which indicates a minor disability. A complete blood count showed leukocytosis (13,000/mm3). Urgent computed tomography (CT) of the brain detected a 4.2 × 2.3 × 4.3-cm abscess at the left temporal lobe (figure 2) and a breach of the tegmen tympani. CT also showed cerebral edema, a midline shift to the right, and bony erosion at the lateral aspect of the right mastoid bone.
The patient underwent an emergency burr-hole aspiration of the abscess. During the procedure, neurosurgeons obtained approximately 40 ml of pus for bacteriologic culture, which grew Proteus mirabilis and Streptococcus milleri. The patient was administered a 6-week course of multiple antibiotics that was designed according to the sensitivity pattern of the organisms. As for the right ear, the cholesteatoma was removed with regular ear toilet.
Some 6 weeks later, the patient underwent a left modified radical mastoidectomy to eradicate the primary focus of cholesteatoma. Cholesteatoma and granulation tissue were removed from the mastoid cavity and middle ear, and the bony plate separating the mastoid antrum and the dura (tegmen tympani) was found to be eroded by the disease. Because the right ear had some residual hearing, the mastoid fistula was treated conservatively with regular suction to remove the keratin debris. Still, pure-tone audiometry revealed a profound mixed hearing loss bilaterally.

At presentation, examination reveals a right-sided post-auricular fistula.
The patient was discharged home after surgery with no neurologic sequelae. Postoperative follow-up CT showed a complete resolution of the abscess. No discharge from the mastoid fistula was seen after removal of the cholesteatoma, and there was no sign of subperiosteal abscess.
Discussion
Otogenic brain abscesses are rare, but when they do occur, the unsafe type of CSOM is a common cause. 3 The most common mechanism of brain abscess is direct extension of an infection through osteitic bone.
In view of the life-threatening potential of this condition, it is important to be aware of the early clinical signs and symptoms. Clinicians should be suspicious of an otogenic brain abscess when confronted with a patient exhibiting headache, giddiness, ataxia, slurred speech, fever, and/or drowsiness in the context of a history of a recurrent, foul-smelling, purulent ear discharge. Other possible signs and symptoms include aphasia, vomiting, and a deterioration in the patients level of consciousness. 4 CT of the brain is warranted. 5
Temporal lobe abscesses are more common than cerebellar abscesses. In a study of 41 otogenic brain abscesses, Sennaroglu et al reported that 22 (54%) were located in the temporal lobe, 18 (44%) were in the cerebellum, and 1 (2%) was in both locations. 4 Temporal lobe abscesses usually involve a defect in the tegmen tympani, 4 as occurred in our patient.
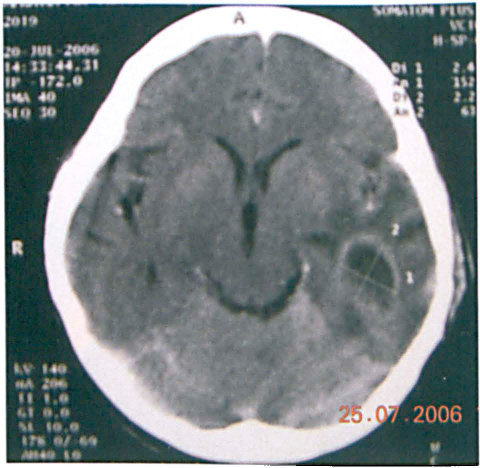
CT shows the abscess in the left temporal lobe.
In our case, we isolated two organisms: P mirabilis and S milleri. In a study of 33 otogenic brain abscesses, Penido Nde et al found that 6 (18%) were caused by P mirabilis and 2 (6%) by S milleri. 6 On the other hand, Ludman found that the most common microorganisms in otogenic brain abscess were streptococci. 2
Mastoid fistulae usually occur in association with a subperiosteal abscess and cholesteatoma. 7 However, in our patient, the mastoid fistula was not discharging and the right ear was clean after treatment of the cholesteatoma.
In our case, clinical suspicion and CT of the brain led to an early diagnosis of the temporal lobe abscess. High doses of fourth-generation broad-spectrum antibiotics and early neurosurgical intervention followed by a modified radical mastoidectomy helped to save the life of our patient.