
Abstract

The internal jugular vein (IJV) is a delicate vessel that is well protected by deep fascia. Still, it is at risk of injury during neck dissection. While head and neck surgeons are well trained to avoid and manage major vascular injuries, some rare anatomic variations of major vessels can pose problems for even experienced surgeons. We encountered a rare variation of an IJV that we found incidentally during a neck dissection.
The patient was a 40-year-old man with a squamous cell carcinoma of the lateral border of the tongue who was undergoing a hemiglossectomy with elective neck dissection under general anesthesia. Profuse venous hemorrhage occurred during dissection of the carotid and submandibular triangles. Complete hemostasis was achieved by ligating the bleeding vessel, but further dissection revealed injury to the fenestrated IJV (figure 1). The vessel was repaired meticulously. Another small fenestration was found about 1 cm cranially (figure 2). The common facial vein was joining the normal part of the IJV present between these two fenestrations, while other veins were draining in the anterior part of the second (lower) fenestration of the IJV. The spinal accessory nerve was found passing above the IJV. The remainder of the procedure was uneventful, and the patient recovered well.
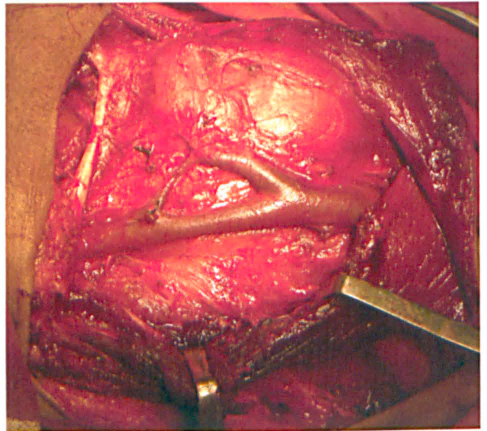
Intraoperative photograph shows the IJV variation.
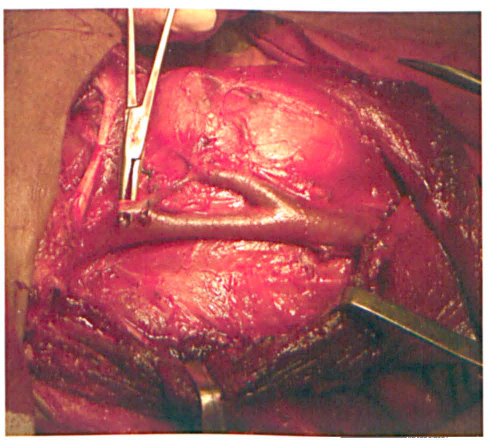
A hemostatic clamp is introduced into the upper fenestration.
Duplication and fenestration are rare variations of IJV anatomy. The reported incidence of duplication is 0.4%, 1 and the incidence of fenestration is likewise less than 1%.2,3 In cases of duplication, the IJV splits into two parts just below the jugular foramen, and the vessels drain separately into the subclavian vein. IJV fenestration is always associated with the passing of the spinal accessary nerve through the fenestration. Fenestration is commonly found in the upper one-third of the IJV. It is similar to duplication except that both segments reunite to form a single vessel before joining the subclavian vein. These two variations are also associated with aneurysm and phlebectasia.
Three mechanisms—vascular, neural, and osseous—have been suggested to explain the development of these variations; the vascular hypothesis is the most widely accepted.1,4–7 To the best of our knowledge, only 15 cases of IJV fenestration have been reported in the literature,7–9 and no case of a double fenestration of the same IJV has ever been reported until now.
Head and neck surgeons should be aware of IJV variations. Any vascular injury (as occurred in our case) must be repaired meticulously or else venous pressure may lead to ligature slippage and postoperative hemorrhage.