Abstract
A 50-year-old woman, a music teacher, presented with a 6-month history of dysphonia. Her symptoms began while she was recovering from a respiratory illness. She also complained of voice fatigue and odynophonia. On examination, her voice was weak, breathy, and mildly raspy.
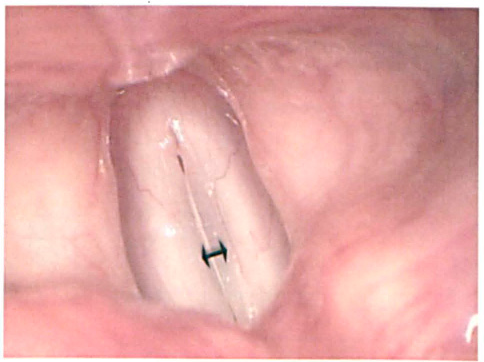
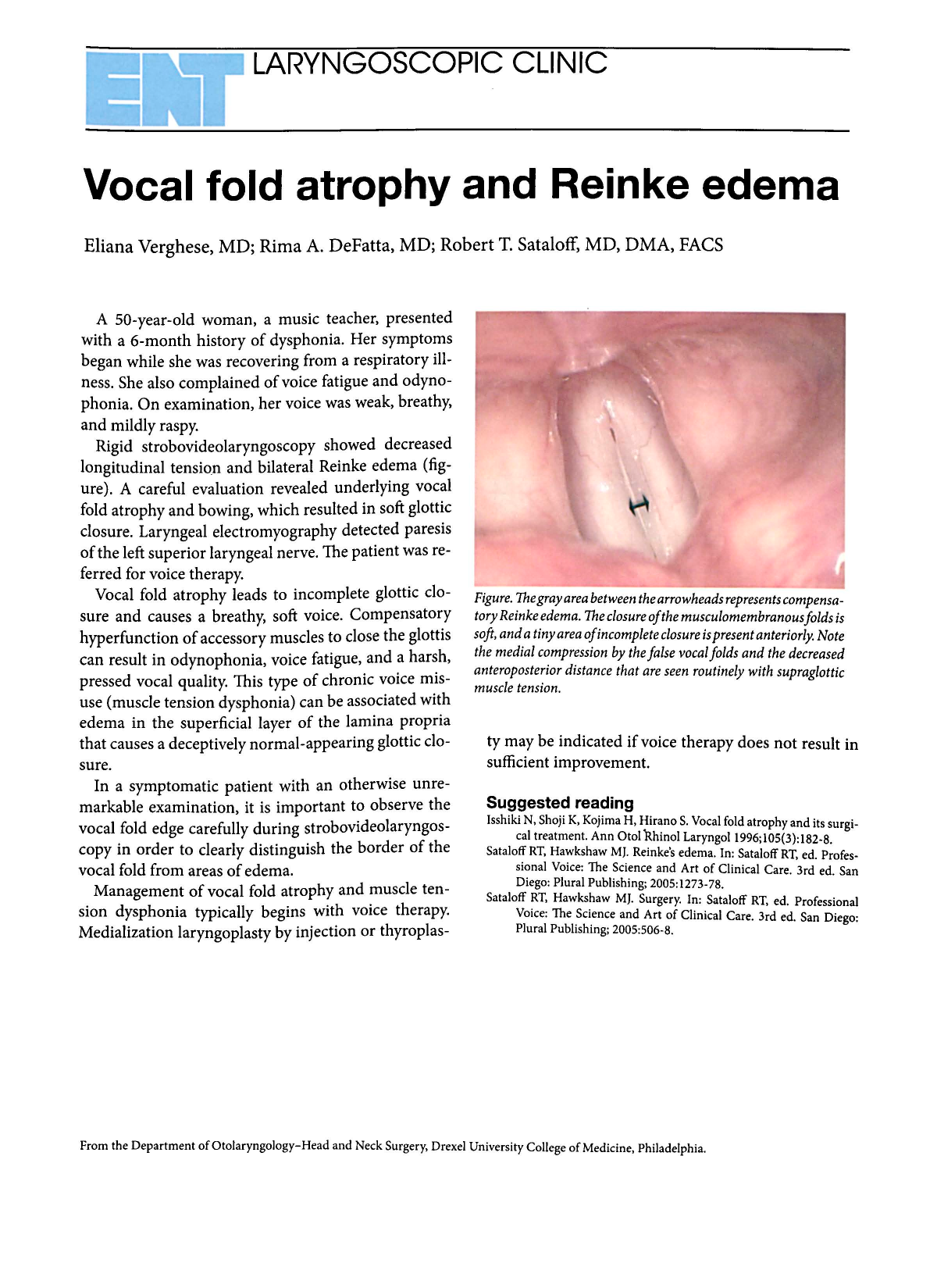
Rigid strobovideolaryngoscopy showed decreased longitudinal tension and bilateral Reinke edema (figure). A careful evaluation revealed underlying vocal fold atrophy and bowing, which resulted in soft glottic closure. Laryngeal electromyography detected paresis of the left superior laryngeal nerve. The patient was referred for voice therapy.
Vocal fold atrophy leads to incomplete glottic closure and causes a breathy, soft voice. Compensatory hyperfunction of accessory muscles to close the glottis can result in odynophonia, voice fatigue, and a harsh, pressed vocal quality. This type of chronic voice misuse (muscle tension dysphonia) can be associated with edema in the superficial layer of the lamina propria that causes a deceptively normal-appearing glottic closure.
In a symptomatic patient with an otherwise unremarkable examination, it is important to observe the vocal fold edge carefully during strobovideolaryngoscopy in order to clearly distinguish the border of the vocal fold from areas of edema.
Management of vocal fold atrophy and muscle tension dysphonia typically begins with voice therapy. Medialization laryngoplasty by injection or thyroplasty may be indicated if voice therapy does not result in sufficient improvement.
Figure. The gray area between the arrowheads represents compensatory Reinke edema. The closure of the musculomembranous folds is soft, and a tiny area of incomplete closure is present anteriorly. Note the medial compression by the false vocal folds and the decreased anteroposterior distance that are seen routinely with supraglottic muscle tension.