
Abstract
We conducted a prospective study to compare the effectiveness of conventional computed tomography (CT) and puffed-cheek CT in detecting the presence and extension of oral cavity malignant tumors. We enrolled 11 patients—5 men and 6 women, aged 32 to 85 years—who had a primary squamous cell carcinoma of the oral cavity. These tumors were located in the floor of the mouth in 4 patients, in the buccal mucosa in 4, in both the buccal mucosa and retromolar trigone in 2, and in the retromolar trigone only in 1. First, conventional contrast-enhanced axial CT was obtained through the oral cavity and neck in each patient. Next, axial imaging was obtained through the oral cavity while patients inflated their cheeks, pursed their lips, and held their breath. We found that the puffed-cheek CTs provided more information regarding the size and extent of the squamous cell carcinomas than did the conventional CTs. For example, in 8 patients, conventional CT could not differentiate the tumor from the normal mucosal surface, but puffed-cheek images clearly showed the surface of the tumor as distinct from the normal mucosa. More disconcerting was the fact that in the other 3 patients, conventional CTs were evaluated as normal, even though puffed-cheek imaging clearly showed the mass in each case. We conclude that puffed-cheek CT is superior to conventional CT for evaluating the mucosal surfaces of the oral cavity. It provides a clearer and more detailed picture with no downside.
Introduction
Clinical examination often “understages” the deep spread of oral cavity tumors. 1 Computed tomography (CT) provides additional staging information that helps determine more precisely the exact local extent of a tumor. Moreover, CT helps in nodal staging at the same time. However, because the mucosal surfaces, the muscle tissues, and the surrounding facial planes in the oral cavity are in close relationship with each other, it is usually difficult to delineate anatomic structures by conventional CT alone.2,3 For example, small mucosal tumors of the oral cavity are usually not visible on conventional CT. Although large, bulky tumors are apparent, CT cannot always identify their surface of origin.3,4
It has been previously shown that dynamic maneuvers that distend a normally collapsed lumen make it easier for clinicians and radiologists to examine the upper aerodigestive tract.5,6 Likewise, distension of the oral cavity during CT has been shown to facilitate the detection of small tumors and to provide information on their extent.7–9 Distension of the oral cavity for CT is indicated when the apposition of the surface of the buccal mucosa and the surface of the gingival mucosa hinders localization and demonstration of tumor extent. It may also be useful when the mucosal surfaces of the tongue and the gingival mucosa are apposed.
In an effort to add to our knowledge of puffed-cheek CT, we conducted this study to compare its effectiveness with that of conventional CT in the evaluation of oral cavity tumors.
Patients and methods
For this prospective study, we enrolled 11 patients—5 men and 6 women, aged 32 to 85 years—with a histologic diagnosis of primary squamous cell carcinoma of the oral cavity. Four of these tumors were located in the floor of the mouth, 4 in the buccal mucosa, 2 in both the buccal mucosa and retromolar trigone, and 1 in the retromolar trigone only. Each patient underwent conventional contrast-enhanced axial CT through the oral cavity and neck followed by puffed-cheek CT through the oral cavity.
We used the puffed-cheek technique described by Weissman and Carrau. 8 Patients inflated their cheeks, pursed their lips, and held their breath. The scanning range extended from the infraorbital line to the inferior edge of the mandible. For continuous imaging, the scanning equipment was set to 120 kV, 90 to 110 mA, 5-mm thickness, and 5-mm table movement (HiSpeed CT; GE Healthcare; Little Chalfont, England; and Hitachi W950 SR CT; Hitachi Medical Corp.; Tokyo). The same radiologist (N.E.) interpreted all CTs.
Results
Three patients in whom puffed-cheek CT clearly showed a mass were found to have no abnormality on conventional CT (figures 1 and 2). Two of these patients had a buccal mucosa tumor and 1 had a retromolar trigone tumor.
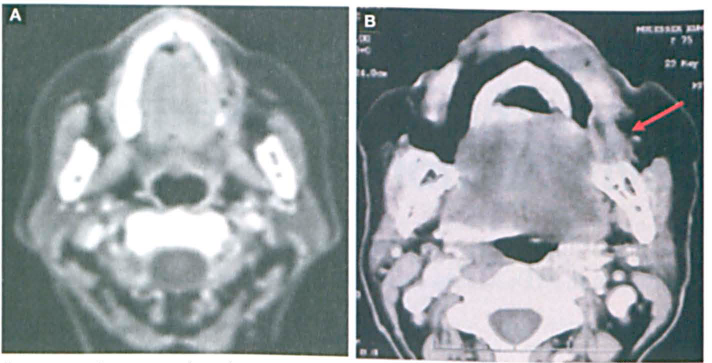
A: Conventional axial CT does not clearly demonstrate the tumor in this patient with a squamous cell carcinoma of the left buccal mucosa. B: With the puffed-cheek technique, the tumor (arrow) is clearly visible.
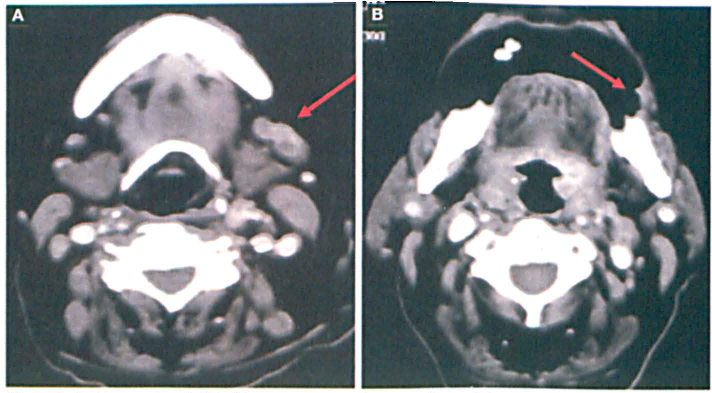
A: Conventional CT of the same patient shown in figure 1 demonstrates multiple enlarged and necrotic submandibular lymph nodes (arrow). B: The puffed-cheek CT shows not only buccal mucosa involvement, but a decreased expansion capacity of the cheek (arrow), as well.
In the other 8 patients, conventional CT showed a mass in the oral cavity, but it could not differentiate the mass from the normal mucosal surface. The puffed-cheek images clearly showed which surfaces harbored tumor involvement (figure 3).
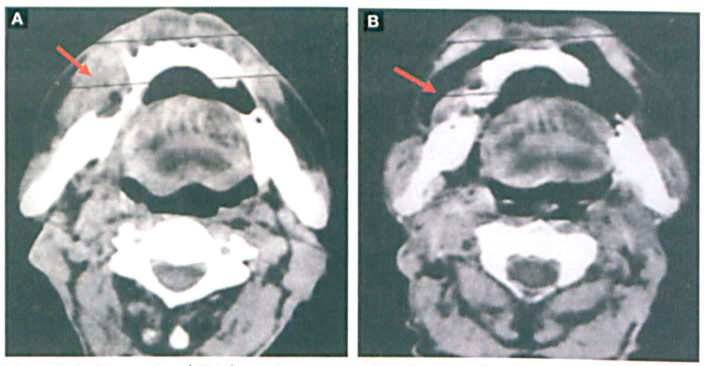
A: Conventional CT shows the tumor eroding the arcus alveolaris mandibulae (arrow), but it is unclear whether there is involvement of the tongue and buccal-masseteric tissue, B: The puffed-cheek CT shows that the tumor (arrow) has not affected the tongue or the mucosal surface of the cheek.
In all 11 cases, puffed-cheek studies showed the location, size, and extent of the tumor better than conventional CT did. All patients were treated successfully with surgery.
Discussion
Since the oral cavity is highly accessible to clinical examination, radiologic studies are not a primary diagnostic tool. 3 Visual inspection and bimanual palpation are the cornerstones of the diagnosis of oral cavity disease. 10 However, it is possible to miss or underestimate pathologic processes in the gingival and buccal mucosa on clinical examination. 11
CT studies complement the clinical examination by delineating deep extension of tumors and by identifying metastatic cervical lymphadenopathy. However, a major limitation of CT examinations of oral cavity tumors is that lesions cannot be easily outlined by conventional CT because of the proximity of anatomic structures to each other. Apposition of two mucosal surfaces limits our ability to determine from which surface a tumor has originated. The surfaces of the oral cavity that are often in contact are the buccal mucosa, the labial mucosa, and the alveolar mucosa of the mandible and maxilla.
Dynamic maneuvers such as puffed-cheek distension combined with breath holding can facilitate a better delineation of lesions that have indistinct margins and irregular contours. During puffed-cheek CT of the oral cavity, air separates the mucosal surfaces, which may allow the radiologist to identify a tumor's location when the location might not otherwise be known.
Structures that are normally apposed—such as the cheeks, gingiva, lips, and buccal vestibule—are well depicted on puffed-cheek CT. The buccinator muscle, pterygomandibular raphe, and retromolar trigone are well delineated with cheek distension, and the location of a tumor on the buccal mucosa or gingival mucosa is clearly identified.
Another helpful maneuver is to have the patient move the tongue away from the palate and gingiva before inflating the cheeks, which allows the radiologist to distinguish the tongue from the floor of the mouth and from the gingiva. The gingiva can also be distinguished from the lip.
Another advantage of cheek distension is that the degree of expansion capacity in the presence of a lesion provides additional information about the cheek's rigidity secondary to infiltration.
Filling the oral cavity with air by cheek distension is easy to do, it costs nothing, and the extra time required is negligible. Bredesen et al reported that 53 of 54 patients in their series were able to perform cheek distension in accordance with a recorded voice instruction. 2 Our patients were asked to suspend respiration for the duration of the maneuver, and all were able to comply.
To fashion a brief and tailored study, we chose precise scanning locations for the conventional CT images. Although puffing the cheeks caused some flattening of the buccal fat pad, the anatomic structures related to the buccal space—such as the zygomaticus major muscle, the parotid duct, and the facial vein—were all equally visible on both series of scans.
In conclusion, we found that puffed-cheek CT allowed for a clearer and more detailed evaluation of the mucosal surfaces of the oral cavity than did conventional CT. While standard CT can be insufficient for identifying tumor location, imaging during distension may contribute to a more exact localization.
The puffed-cheek technique can allow radiologists to detect small primary tumors and to delineate tumor margins better than they can with conventional CT. For selected patients with suspected tumor involvement of the buccal vestibule or adjacent area, puffed-cheek CT may serve as a worthy supplement to conventional CT.
Although our study sample was small, we believe that our findings contribute to the existing literature and to daily clinical practice.