
Abstract
We report our experience with hyoid suspension surgery in patients with obstructive sleep apnea (OSA) diagnosed on the basis of polysomnographic criteria. We conducted a prospective, observational study of 20 patients—18 males and 2 females, aged 15 to 52 years (mean: 42. 1)—who were treated at our tertiary care center. All patients underwent hyoid suspension surgery and uvulopalatopharyngoplasty (UPPP) in a single session. Postoperative success was defined as either (1) a reduction in the apnea-hypopnea index (AHI) from 20 or higher to less than 20 or (2) a reduction in AHI of at least 50%. Postoperative follow-up polysomnography indicated that surgery was successful in 18 of 20 patients (90%). No important complications were observed. We conclude that hyoid suspension surgery is an effective procedure with low morbidity for the treatment of OSA in selected patients with hypopharyngeal obstruction. We believe it is a good option for those patients who will not or cannot tolerate therapy with continuous positive airway pressure.
Introduction
Obstructive sleep apnea (OSA) is clinically defined by frequent episodes of apnea and hypopnea during sleep. OSA is a serious disorder that has been implicated in extreme daytime hypersomnolence, functional impairment, and automobile accidents.1–3 It is also associated with cardiovascular morbidity and mortality secondary to hypertension, congestive heart failure, cardiac arrhythmia, myocardial infarction, and cerebrovascular disease.1–3
Sleep apnea is defined as a complete cessation of oronasal airflow for a minimum of 10 seconds, and hypopnea is defined as a reduction in oronasal airflow of at least 50% accompanied by a decrease of more than 3% in ongoing arterial oxygen pressure (PaO2). 4 The apnea-hypopnea index (AHI), also known as the respiratory disturbance index, is the sum of the number of apneic and hypopneic events per hour during sleep, and it indicates the severity of OSA.
The estimated prevalence of OSA is 2% of women and 4% of men aged 30 to 60 years. 5 Male sex and obesity are strongly associated with OSA. 5 Other risk factors include increased neck circumference, craniofacial abnormalities, hypothyroidism, and acromegaly. 6
Management options include medical and surgical treatment. Weight loss, avoidance of sleep in the supine position, and avoidance of sleep medications and sedatives might reduce the severity of OSA, but implementation of these lifestyle alterations often fails. 7 Although the most effective treatment is nighttime ventilation therapy with continuous positive airway pressure (CPAP), 8 the long-term compliance rate with CPAP is less than 70%. 9
For surgery to be as successful as CPAP, the obstruction level of the airway should be precisely identified, and the surgery should be planned accordingly. The most common surgical procedure for OSA is uvulopalatopharyngoplasty (UPPP). 10 A meta-analysis by Sher et al found that the success rate of UPPP was 41%, although it was as low as 5% in patients with excessive retrolingual collapse observed during endoscopy. 11 In the latter case, a mandibular repositioning appliance may be used as a noninvasive treatment for patients with mild or moderate OSA in order to gain retrolingual space. 12 In cases of noncompliance with such an appliance or for patients with more severe OSA, hyoid suspension surgery can be considered.
The goal of hyoid suspension surgery is to stabilize the hyoid bone inferiorly and anteriorly on the superior border of the thyroid cartilage. When this is achieved, the posterior airway space is widened and the tongue base obstruction is minimized. Hyoid suspension surgery is less invasive than the more widely used genioglossus advancement with hyoid myotomy. However, the outcomes of hyoid suspension surgery have been reported in only a few studies.7,13
In this article, we describe our study of hyoid suspension surgery with UPPP as a one-stage multilevel surgical procedure in patients with OSA as determined by objective polysomnographic criteria.
Patients and methods
We conducted a prospective, observational study of 20 patients with OSA—18 males and 2 females, aged 15 to 52 years (mean: 42.1)—who underwent hyoid suspension surgery along with UPPP from March 2002 through September 2007 at Ankara University Hospital. All patients had previously been offered CPAP as an alternative, but they either refused to try it or failed to adequately comply with the regimen.
All patients were initially evaluated by a detailed history and complete otolaryngologic examination. Their body mass index ranged from 23 to 28 (mean: 26.0). The diagnosis of OSA was based on overnight polysomnography results. (For 2 patients with nasal pathology, polysomnography was undertaken after nasal surgery was performed; both underwent septoplasty, 1 with and 1 without inferior turbinate reduction.)
The complete polysomnographic investigation included electroencephalography, chin and leg electromyography, airflow monitoring, thoracic and abdominal respiratory effort, and pulse oximetry. The AHI was calculated as the mean sum of obstructive apneas and hypopneas per hour during sleep. Obstructive apnea was defined as a complete cessation of oronasal airflow for a minimum of 10 seconds, and hypopnea was defined as a reduction in airflow of 50% or more accompanied by a decrease of more than 3% in ongoing PaO2.
The degree of OSA was categorized as either mild (AHI: 5 to 14), moderate (15 to 29), or severe (≥30). 4 Preoperative AHI scores ranged from 11 to 84 (mean: 31.0). Polysomnography revealed that 1 patient (5%) had mild OSA, 12 (60%) had moderate OSA, and 7 (35%) had severe OSA. Clinically, all patients were categorized as Friedman stage I (high-risk oropharyngeal obstruction). Table 1 shows individual characteristics according to the category of OSA, and table 2 shows group pre- and postoperative AHIs by category.
Individual data according to the degree of OSA preoperatively
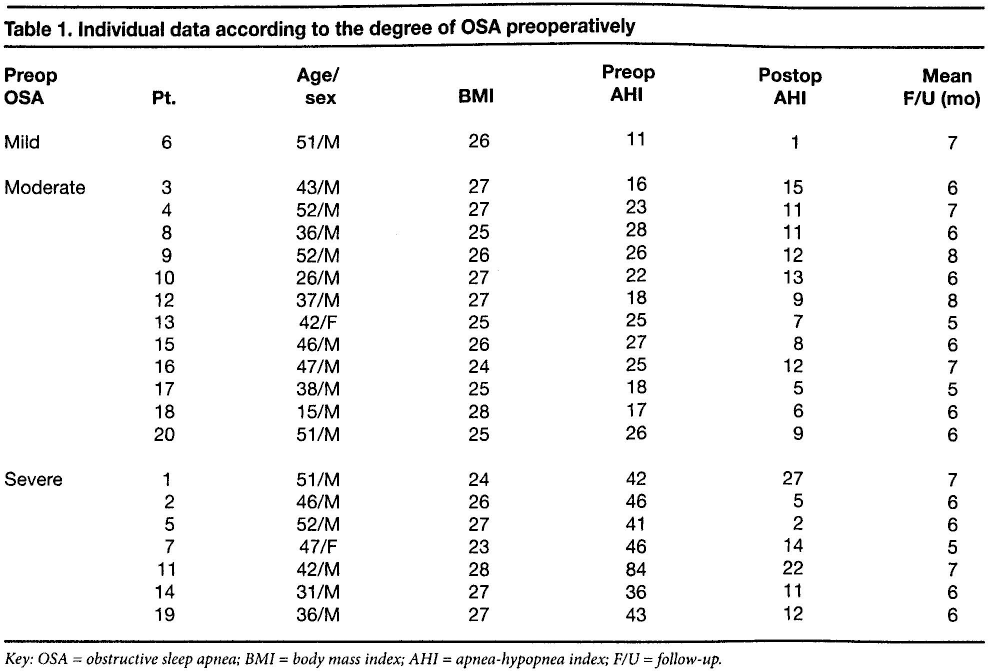
Key: OSA = obstructive sleep apnea; BMI = body mass index; AHI = apnea-hypopnea index; F/U = follow-up.
Hyoid suspension surgery was performed in the manner described by Hormann and Baisch, 14 and UPPP was also performed. The criterion for surgical success was either (1) a reduction in the apnea-hypopnea index (AHI) from 20 or higher to less than 20 or (2) a reduction in AHI of at least 50%.
Results
Patients underwent monthly follow-up, and repeat polysomnography was performed between 5 and 8 months postoperatively (mean: 6.3). Based on our criteria for success, surgery was successful in 18 of the 20 patients (90%). One of the 2 patients with an unsuccessful outcome had moderate OSA both pre- and postoperatively, and the other improved from severe to moderate OSA. Overall, the mean postoperative AHI fell from 31.0 to 10.6 (tables 1 and 2). A total of 11 patients improved from moderate to mild, 5 improved from severe to mild, and 2 improved from severe to moderate.
Distribution of mean pre- and postoperative AHIs according to the degree of OSA by group
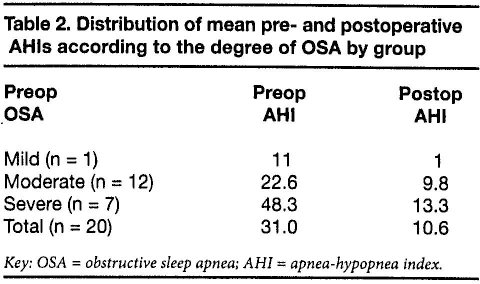
Key: OSA = obstructive sleep apnea; AHI = apnea-hypopnea index.
No important complications were observed. A mild, transient aspiration was seen in 2 patients (10%) during postoperative week 1, and only minimal pain was reported by all patients during postoperative days 1 to 5.
Discussion
Lin et al reported that 24% of OSA patients who required CPAP were lost to follow-up after their initial polysomnography. 15 The authors noted that earlier studies of CPAP compliance did not generally take into account those patients who failed to even begin CPAP after initial PAP titration. Lin et al also reported that 69% of patients who discontinued or never began CPAP were not aware of other treatment options, and that 75% of these patients said they would be interested in learning more about surgical alternatives to CPAP for treatment of their OSA. 15
Hypopharyngeal obstruction has been treated with many different approaches. Improvement of the hypopharyngeal airway by intervention at the level of the hyoid complex was first demonstrated in animal models. In 1983, Patton et al demonstrated that expansion of the hyoid arch resulted in increased hypopharyngeal airspace in dogs. 16 In another canine experiment the next year, Van de Graaff et al reported that the hyoid arch and the attached muscles affected upper airway resistance and patency; they also found that anterior replacement of the hyoid arch resulted in a significant reduction in resistance. 17 Surgical intervention at the hyoid complex in humans was introduced by Kaya 18 and later described by Patton and Thawley 19 and Riley et al. 20
Worldwide, hyoid suspension surgery is usually performed along with genioglossus advancement or maxillomandibular osteotomy.21–25 Riley et al reported a success rate of 61% for genioglossus advancement with hyoid myotomy plus UPPP. 20 Later, Neruntarat reported successful outcomes of 81% in the short term and 65% over the long term with genioglossus advancement and hyoid myotomy. 23 By performing hyoid suspension surgery without genioglossus advancement or maxillomandibular osteotomy, the surgeon can significantly reduce the invasiveness of the operation.
Baisch et al reported a 59.7% success rate in a series of 67 patients who were treated with multilevel surgery, including hyoid suspension. 13 Neruntarat reported a 78% success rate in patients treated with hyoid suspension and a uvulopalatal flap under local anesthesia. 24 In a study of hyoid suspension as a one-stage multilevel procedure in 22 patients, Richard et al reported an overall success rate of 72%, with no difference in outcomes between patients who did and did not undergo genioglossus advancement. 26
On the other hand, Bowden et al reported a success rate of only 17% with hyoid suspension and UPPP in their study of 29 patients with mild to severe OSA. 27 Finally, a study by den Herder et al found that hyoid suspension alone was successful in 71% of patients with moderate to severe OSA. 7
Our experience with this one-stage multilevel surgery yielded a 90% success rate, which is higher than success rates previously reported by others using a similar multilevel surgery approach, similar patient selection criteria, and the same criteria for success.7,13,24,26,27
One pitfall of our study is the lack of long-term follow-up results. Another is the possibility that the contribution of UPPP to the success of surgery might have been underestimated. Further studies with larger patient populations are needed.
In conclusion, hyoid suspension surgery is an effective procedure with low morbidity for the treatment of selected OSA patients with hypopharyngeal obstruction. This procedure is a worthwhile option for patients who will not or cannot tolerate CPAP.