
Abstract
We conducted a 3-year retrospective study to examine the results of preoperative hematologic screening, the incidence of postoperative bleeding, and the possible relationship between the two factors in patients who had undergone tonsillectomy with or without adenoidectomy. Our study population was made up of 875 patients—441 boys and 434 girls, aged 2 to 18 years (mean: 7.52 ± 4.25)—who had been treated at our institution from January 2004 through December 2006. In addition to demographic data, we compiled information on each patient's medical and surgical history, personal and family history of abnormal bleeding, indication for tonsillectomy, and preoperative hematologic screening results. The latter included determinations of the prothrombin time, activated partial thromboplastin time, international normalized ratio (INR), and platelet count. A total of 748 patients (85.5%) had normal findings on preoperative hematologic screening, and 127 (14.5%) had at least one abnormality. Postoperatively, hemorrhagic complications occurred in 31 children (3.5%)—in 22 of the 748 patients with normal screening results (2.9%) and in 9 of the 127 with a screening abnormality (7.1%); the difference between the two groups was statistically significant (p = 0.041). The abnormalities in the latter group consisted of an elevated INR but no otherwise identifiable coagulopathy. Another 14 patients with an abnormal screening result (11.0%) were found to have at least one coagulopathy that was newly diagnosed during our preoperative evaluation; they were treated perioperatively, and none bled postoperatively. Of 21 patients who had a personal or family history of abnormal bleeding, 5 (23.8%) were found to have a coagulopathy, but none bled following surgery. In conclusion, we found that preoperative hematologic screening identified patients with undiagnosed coagulopathies, and with appropriate treatment our surgeons were able to prevent some bleeding events in these patients. Our finding that patients with a mildly elevated INR had a higher incidence of postoperative hemorrhage warrants further study.
Introduction
Tonsillectomy, one of the oldest surgical procedures, was first described by Celsus in 30 AD. 1 Approximately 300,000 of these procedures are performed in the United States annually. 2 It represents the first surgical experience for most children.
The risk of mortality from tonsillectomy is extremely low, estimated at approximately 1 in 16,000 patients; when death does occur, it is usually associated with hemorrhage, airway obstruction, or complications of anesthesia.3,4 Sandoval et al estimated the incidence of post-tonsillectomy hemorrhage at 4,300 cases annually. 5 According to Burk et al, reported rates of postoperative hemorrhage range from 2 to 7%. 6
Postoperative bleeding is generally characterized as either immediate or delayed. Immediate, or primary, hemorrhage occurs within the first 24 hours after tonsillectomy, and it is generally attributable to incomplete hemostasis during the operation. Delayed hemorrhage occurs beyond the first 24 hours, and it is believed to be caused by sloughing of the eschar in the tonsillar fossa with subsequent exposure of the underlying vessels. 4 Several factors contribute to postoperative bleeding: surgical technique, perioperative infection, and the patient's hematologic status. 7
Although screening for a personal or family history of abnormal bleeding tendencies is a standard component of preoperative hematologic evaluation, the issue of laboratory assessment is more controversial. Many clinicians order a hematologic workup for all patients undergoing surgery, while others reserve laboratory evaluation exclusively for patients at high risk for a bleeding abnormality. Those who do order a laboratory evaluation might do so in order to detect a previously undiagnosed bleeding disorder or to document a patient's hematologic status for medicolegal purposes. 8
According to the American Academy of Otolaryngology-Head and Neck Surgery, a coagulation and bleeding workup is warranted only if an abnormality is suspected by personal or family history or if the family history is unavailable. 9 A body of literature exists that supports routine preoperative laboratory screening for coagulopathy (table 1).10–14 On the other hand, there are also studies that question the efficacy of the laboratory evaluation (table 2),3,4,6,15–18 especially in light of the estimated $30 million cost of preoperative hematologic studies. 19
Summary of studies that support routine preoperative coagulation screening
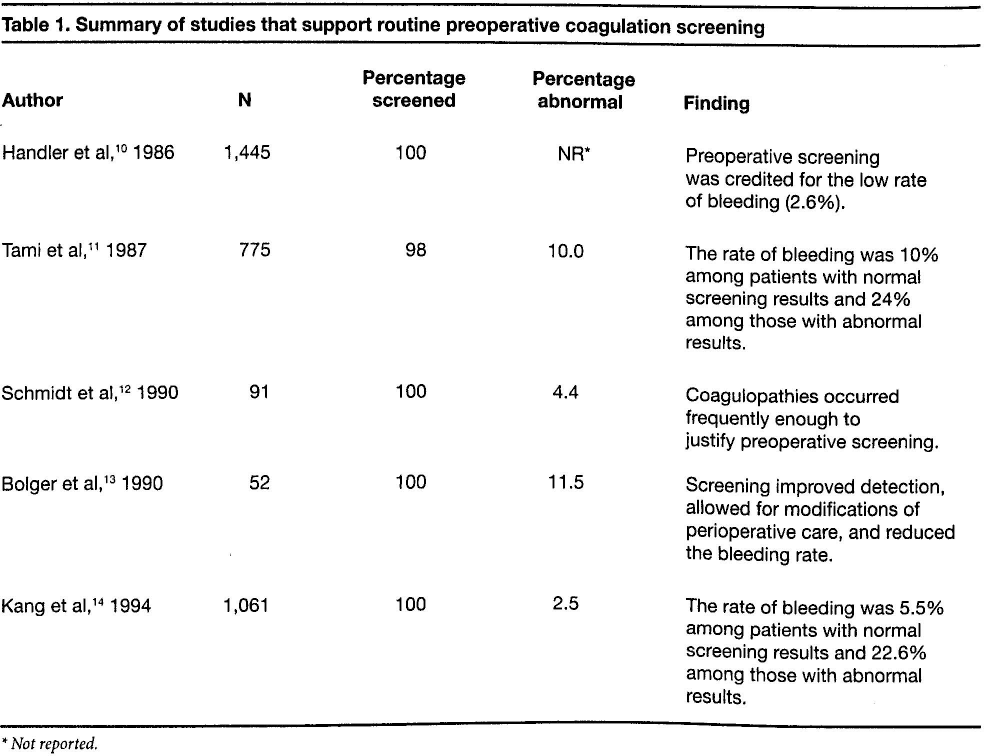
Not reported.
Summary of studies that do not support routine preoperative coagulation screening
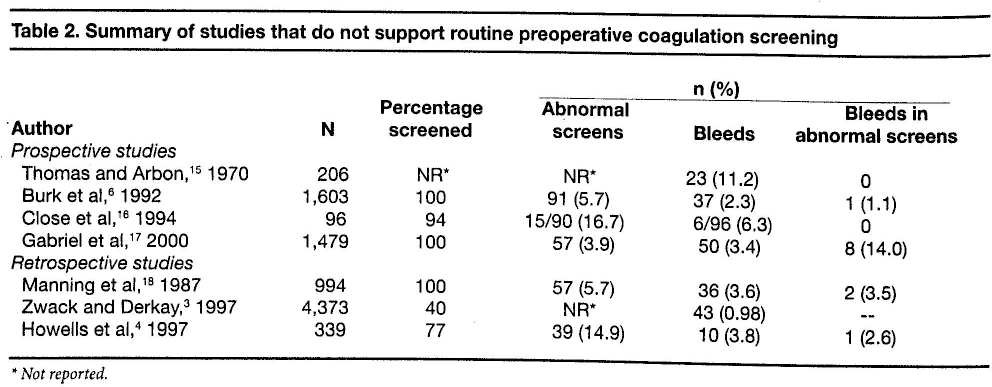
Not reported.
In this article, we describe our own study of the value of a preoperative coagulation workup for children undergoing tonsillectomy.
Patients and methods
We retrospectively reviewed the records 875 children who had undergone tonsillectomy or adenoidectomy at Temple University Hospital from January 2004 through December 2006. This group consisted of 875 patients—441 boys and 434 girls, aged 2 to 18 years (mean: 7.52 ± 4.25). Most of these patients were either black (40.6%), white (32.2%), or Hispanic (23.5%). Their mean body mass index (BMI) was 20.5 (±9.05); 9% of these children had a BMI between 25 and 29.9, and 8% had a BMI of 30 or more.
Preoperative characteristics
In addition to demographic data, we reviewed inpatient and outpatient charts for each patient's medical and surgical history, personal and family history of bleeding, indication for surgery, and preoperative hematologic screening results. The screening included determinations of the prothrombin time (PT), activated partial thromboplastin time (aPTT), international normalized ratio (INR), and platelet count.
Patients who were found to have persistently abnormal preoperative screening results were referred to the hematology service for further evaluation, and those who were subsequently identified as having a coagulopathy were treated perioperatively according to the hematology service's standard guidelines.
Concomitant conditions
Analysis of the medical histories revealed that the most commonly encountered medical conditions at presentation were obstructive sleep apnea (47%), asthma (24%), and inhalant allergies (8%). Some 11% of these patients had previously undergone surgery of some sort—the most common being adenoidectomy (48%), incision and drainage of a peritonsillar abscess (15%), hernia repair (13%), dental procedures (13%), and orthopedic procedures (9%).
Bleeding history
A total of 21 patients (2.4%) had a ersonal or family history of hematologic abnormalities; 10 patients (1.1%) had a personal history of such, and 11 (1.3%) had a family history. A bleeding abnormality was defined as pathologic bleeding or a documented elevation in coagulation parameters. Five of the 21 patients (23.8%) were subsequently diagnosed with a coagulopathy on further laboratory evaluation.
Indications for tonsillectomy
The most common indication for tonsillectomy was obstructive sleep apnea without tonsillitis (65.7%), which had been diagnosed clinically or based on the results of polysomnography. Other common indications included obstructive sleep apnea with tonsillitis (19.5%), recurrent tonsillitis (13.8%), and asymmetric tonsils (0.5%).
Surgical technique
All tonsillectomies were performed by residents under the direct supervision of the attending physician. Each procedure was performed with bipolar scissors electrocautery. When an adenoidectomy was also performed, it was done sharply either with curettage and monopolar suction cautery for hemostasis or with monopolar suction cautery alone. All patients were admitted for postoperative observation for at least 23 hours.
Outcomes
The outcome of each surgery was evaluated with respect to peri- and postoperative hemorrhage. Bleeding was classified as either immediate (<23 hr), early (≥23 hr to <3 days), or late (≥3 days). The three options available to control bleeding were categorized as either none necessary, management at bedside, or return to the operating room.
Results
Findings on hematologic screening
Preoperative hematologic laboratory values were normal in 748 patients (85.5%) and outside the normal range in 127 patients (14.5%). Among the entire study population, elevations in PT, aPTT, and INR were noted in 63 (7.2%), 36 (4.1%), and 106 patients (12.1%), respectively; some of these patients had more than one abnormality (table 3).
Statistically significant and nonsignificant associations in univariate analysis (statistically significant values are in boldface)
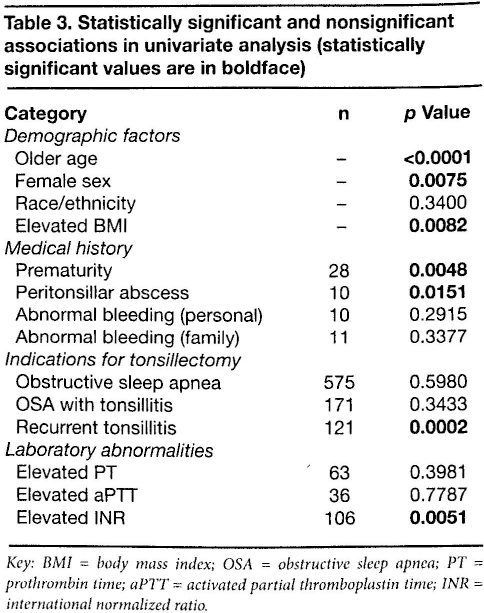
Key: BMI = body mass index; OSA = obstructive sleep apnea; PT = prothrombin time; aPTT = activated partial thromboplastin time; INR = international normalized ratio.
A total of 17 patients (1.9%) who had a persistent hematologic laboratory abnormality were referred to our hematology clinic for further evaluation; 14 of them (1.6% of the entire study population) were diagnosed with at least one blood disorder (table 4), and the other 3 (0.3%) were found to have a virally induced inhibitor. Those patients with a specific clotting factor deficiency were treated accordingly, and 2 patients with von Willebrand disease were given desmopressin. In addition, aminocaproic acid was given when indicated.
Coagulopathies identified and treated in the 14 patients with a persistent coagulation abnormality
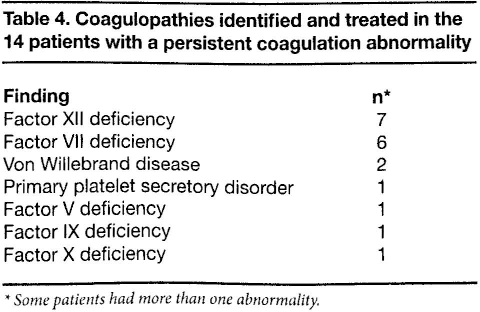
Some patients had more than one abnormality.
Postoperative hemorrhage
There were 31 hemorrhagic complications (3.5%). A total of 22 complications occurred among the 748 patients with a normal preoperative hematologic value (2.9%), and 9 occurred among the 127 patients with an abnormal value (7.1%). The difference between the two groups was statistically significant (p = 0.041).
Of note, in all 9 cases of bleeding in the group with an abnormal screening result, the only identifiable abnormality was an elevated INR. No postoperative hemorrhagic events occurred in any of the 14 patients with other preoperatively identified and treated coagulopathies.
Of the 31 postoperative bleeds, 4 were classified as early and 27 as late. The 27 patients in the latter group required hospital admission, and their bleeding was controlled in the operating room in most cases.
Of the 5 patients with a personal or family history of abnormal bleeding who were subsequently diagnosed with a coagulopathy, none experienced a postoperative bleed.
Statistical analysis of risk factors
A univariate analysis of demographic data and medical and surgical parameters revealed that several factors were significantly associated with an increased risk for post-tonsillectomy hemorrhage: older age, female sex, an elevated BMI, a history of prematurity, a history of peritonsillar abscess, recurrent tonsillitis as an indication for tonsillectomy, and an elevated preoperative INR (table 3).
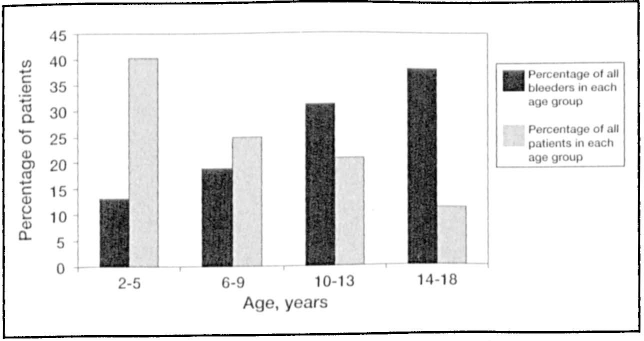
A multivariate analysis of these parameters found that older age (p < 0.0001) (figure), female sex (p = 0.0097), and an elevated INR (p = 0.0181) were independent predictors of postoperative hemorrhage.
Discussion
Comparisons with other studies
As mentioned, the use of preoperative laboratory evaluation to predict hemorrhagic complications has been a subject of debate for many years, and multiple studies have yielded conflicting results. For example, prospective investigations by Close et al 16 and Gabriel et al 17 failed to identify a significant relationship between a clinical history of bleeding and laboratory abnormalities. Our data do not support their conclusions; we found 5 that of 21 patients (23.8%) who had a family or personal history of bleeding were subsequently diagnosed with a coagulopathy by hematologic screening. These patients were treated for their clotting disorder perioperatively, and none of them experienced post-tonsillectomy bleeding.
Figure. Chart demonstrates that older age is an independent predictor of postoperative hemorrhage (p < 0.0001).
Patel et al surveyed members of the Society for Pediatric Anesthesia practicing in North America and found that 45% of institutions routinely screened their tonsillectomy patients for PT and aPTT preoperatively. 8 They found no differences in screening practices between urban and nonurban institutions or between teaching and nonteaching institutions.
In our study, the overall incidence of postoperative bleeding was 3.5%, which is consistent with rates in the previously published literature. The incidence of bleeding was significantly higher in our patients with abnormal preoperative hematologic screening results than in those whose screening results were normal—7.1 and 2.9%, respectively (p = 0.041). However, while this difference was statistically significant, it merely reflected the higher rate of bleeding among patients with an elevated INR and no other identifiable coagulopathy. Since the INR was only mildly elevated in this group (typically 1.2, where 1.1 is the upper limit of normal), these patients did not receive any perioperative treatment with a thrombogenic agent.
Of the 127 patients with an abnormal preoperative coagulation study, 14 (11.0%) were newly diagnosed at the preoperative evaluation with at least one coagulopathy. There were 7 cases of factor XII deficiency, 6 cases of factor VII deficiency, 2 cases of von Willebrand disease, 1 case of primary platelet secretory dysfunction, and 1 case each of a deficiency of factor V, IX, and X. Three other patients were found to have a virally induced anticoagulant.
Lupus anticoagulants cause a prolongation of the aPTT, probably as a result of hypoprothrombinemia induced by antiprothrombin antibodies.20,21 Becton and Stine found that children with lupus anticoagulants in serum were at increased risk for bleeding. 22 Most virally induced antiphospholipid antibodies are transient. However, the time course for their disappearance has not been elucidated fully; reported estimates range widely, from weeks to months to years.20,23
The 14 patients in our study who were found to have a coagulopathy were treated perioperatively in conjunction with the hematology service, and none of them experienced a hemorrhagic event. Only 4 of these patients had a personal or family history of abnormal bleeding, which means that 10 diagnoses would have been missed if screening had been based on the history alone.
Among the entire study population, 21 patients (2.4%) had a personal or family history of abnormal bleeding; 5 of them were subsequently diagnosed with a coagulopathy on further laboratory evaluation, and none of them bled. The difference in the rate of bleeding between patients with a diagnosed coagulopathy (0/14; 0%) and those who were not diagnosed with a coagulopathy (31/861; 3.6%) was not statistically significant (Fisher exact test, p = 0.601).
Among the independent predictors of a postoperative hemorrhagic complication were older age, female sex, and an elevated INR. Our finding of an association between increased risk and older age is concordant with those of Roberts et al 1 and Gabriel et al. 17 However, there is no previously published literature regarding the importance of female sex and elevated INR as risk factors for postoperative hemorrhagic complication. The association between female sex and postoperative bleeding is neither intuitive nor precedented. Perhaps future prospective studies that include an evaluation of this relationship may be helpful in distinguishing a true association from mere chance.
In our study, personal and family histories suggestive of a mild coagulopathy were not significantly accurate predictors of postoperative bleeding. Our finding in this regard is in agreement with those published by other groups.16,17
Overall, our findings are subject to the inherent biases associated with retrospective medical record reviews. However, because of the dramatic nature of the relevant outcome measure (postoperative bleeding), these events are not likely to be missed. Also, the existence of a hospital-based electronic medical record at our institution allowed for reliable detection of patients admitted postoperatively for bleeding. Of course, it is possible that we would not have known right away if a patient had sought treatment for postoperative bleeding at another hospital, but we believe that our postoperative follow-up care would have allowed us to eventually identify any such case.
Cost-benefit analysis
Decisions as to whether hematologic screening prior to tonsillectomy should be routine for all patients or be limited to selected groups of patients (e.g., those with a personal or family history of bleeding or a previously diagnosed bleeding diathesis) are typically based on cost-benefit analyses. The costs of routine screening include the monetary costs of testing, the physical pain endured by patients, parental time and anxiety, and the time and money needed for additional workup of patients with abnormal results. The potential benefits include reductions in monetary costs, emotional trauma, and patient morbidity and mortality associated with bleeding complications.
In order to perform such an analysis in our patient population, we must identify those patients who benefited from universal screening. In other words, we must determine how many patients with a newly diagnosed coagulopathy would not have qualified for preoperative screening based on their personal or family history of bleeding alone. The benefit to this group must then be weighed against the cost involved in screening all patients.
In our study, screening was negative in 748 patients; these patients bled at a rate (2.9%) comparable to rates reported in the existing literature. A total of 113 patients had a positive initial screen and a negative additional workup; this group's perioperative care was thus not altered from the norm. Surprisingly, this group bled at a higher rate than expected rate (8.0%), despite having undergone extensive evaluation.
Fourteen of our patients had abnormal initial screening and a positive additional workup, and their perioperative management was modified in order to prevent bleeding; none of these patients bled. Without routine universal screening, 10 of these 14 patients would not have been screened because their personal or family history would not have warranted it. As it was, 10 of our 875 patients (1.1%) potentially benefited from the special attention during their perioperative management that was made possible by routine universal screening.
Unfortunately, the small number of patients with a diagnosed coagulopathy in our study limits our ability to detect whether identification of the coagulopathy may serve to prevent the bleeding. This explains the lack of statistical significance (p = 0.601) in the difference in bleeding rates between those with and without a preoperatively diagnosed coagulopathy. Therefore, we cannot draw any general conclusion about the efficacy of universal screening in preventing postoperative bleeding.
An interesting question generated by our data is, Does the higher rate of bleeding amongpatients with a mildly elevated INR and an otherwise negative hematologic workup truly reflect an increased risk of postoperative bleeding? A prospective study in which investigators randomize this subgroup of patients into two groups—with one group receiving some additional prothrombotic agent as part of their perioperative treatment regimen—may help to answer this question.