
Abstract
During surgical treatment of a patient with otosclerosis, the probability of success depends in large part on the extent of the surgeon's experience. Therefore, predicting the preoperative severity of disease may help determine the choice of surgeon based on how experienced the surgeon should be. We conducted a study to evaluate the relationship between hearing thresholds and footplate thickness in otosclerosis patients who underwent stapes surgery. We used a qualitative method for measuring footplate thickness that was based on the simplicity or difficulty of opening the footplate. Our study population was divided into two groups; group 1 was made up of 66 patients whose footplates were easily opened with low pressure or with repeated motions by hand, and group 2 was made up of 14 patients whose footplate was either opened by drilling or not opened because it had been obliterated. We found that the patients in group 2, who had more severe disease, had significantly higher air-and bone-conduction thresholds than did the patients in group 1. According to our findings, otosclerotic patients with high air- and bone-conduction thresholds generally have more severe disease and thus require a more experienced surgeon.
Introduction
Otosclerosis is the most common cause of conductive hearing loss in the presence of an intact tympanic membrane among patients aged 15 to 50 years.1,2 Otosclerosis can be a factor in the conductive, sensorineural, and mixed types of hearing loss.2,3 Sensorineural hearing loss is caused by the hyalinization of the spiral ligament adjacent to the otosclerotic focus, which affects the otic capsule in such a way that it interferes with the function of the organ of Corti.4,5
According to many authors, the success of surgery for the treatment of otosclerosis depends more on the surgeons experience than on the actual technique itself, and some have cast doubt on the adequacy of residents’ training in stapes surgery.6–9 Regardless of which technique is used, a good surgical result is achieved with the closure of the air-bone gap to 10 dB or less; the risk of further sensorineural hearing loss in the operated ear as a complication of the surgery is less than 1%.7,10 The term “very far-advanced otosclerosis” was proposed by Iurato et al to indicate disease severity in patients whose air-and bone-conduction thresholds are both undetectable by standard clinical audiometry (“blank audiogram”). 11
In this article, we describe our study to evaluate the relationship between hearing thresholds and stapes footplate thickness in otosclerotic patients.
Patients and methods
We conducted a cross-sectional study of patients who had undergone unilateral stapes surgery at Amir-Alam academic hospital in Tehran from May 2005 through February 2006. Inclusion criteria were a primary stapedectomy or stapedotomy that was performed by an experienced surgeon and a chart that contained all the clinical, surgical, and audiologic information.
Our study group was made up of 80 patients—42 women and 38 men, aged 16 to 57 years (mean: 34.0); the mean ages of the women and men were 34.7 and 33.1 years, respectively. Surgery was performed in the right ear in 41 patients and in the left ear in 39 patients.
All patients had undergone preoperative audiometry, and air- and bone-conduction thresholds were obtained from 250 to 8,000 Hz. We then calculated the mean thresholds at 500, 1,000, 2,000, and 4,000 Hz. Mean preoperative air-bone gaps were calculated by subtracting bone-conduction thresholds from air-conduction thresholds at 500, 1,000, 2,000, and 4,000 Hz. We also calculated the Carhart notch for each patient; this value represents the increase in the bone-conduction threshold with the largest depression at 2,000 Hz in the audiometric curve. 2
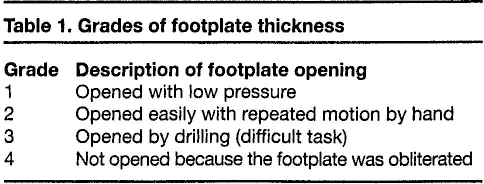
Footplate thickness was jointly determined by three expert surgeons, who assigned one of four grades to each case (table 1). There were 33 patients classified as grade 1, 33 as grade 2, 10 as grade 3, and 4 as grade 4 (table 2). Once each case was graded, the surgeons agreed on the main principles and steps of surgery in order to match the technique to the surgeon. Later on, after the surgical portion of the study had been completed, the surgeons agreed to further classify footplate thickness into two larger groups in order to minimize inter- and intraobserver biases. Therefore, patients with grade 1 and 2 footplates were designated as group 1 and those with grade 3 and 4 footplates were designated as group 2.
Grades of footplate thickness
Distribution of footplate thickness according to sex

For statistical analysis, the Student t test, the z-test, the Fisher exact test, and the chi-square test were used to evaluate all data.
Results
Age and sex
The mean ages of the patients in group 1 and group 2 were 33.6 and 35.4 years, respectively—not a significant difference (p = 0.58). Nor was there a significant relationship between sex and the grade of footplate thickness (p = 1.00) (table 2).
Hearing thresholds
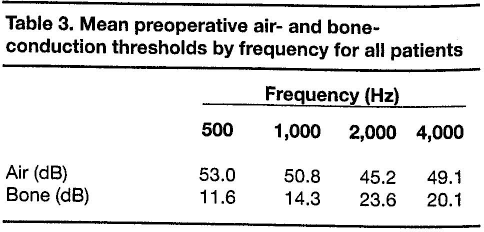
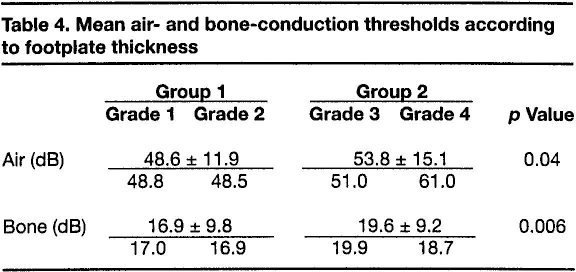
The mean preoperative air- and bone-conduction thresholds for all patients are shown in table 3, and the breakdown of thresholds for both groups and all four grades is shown in table 4. When analyzed by group, the mean air-conduction threshold was 48.6 dB in group 1 and 53.8 dB in group 2, a statistically significant difference (p = 0.04). The mean bone-conduction thresholds in the two groups were 16.9 and 19.6 dB, respectively, which represents another significant difference (p = 0.006).
Mean preoperative air- and bone-conduction thresholds by frequency for all patients
Mean air- and bone-conduction thresholds according to footplate thickness
Some 70% of our patients who had an air-conduction threshold greater that 52 dB had a grade 3 footplate thickness.
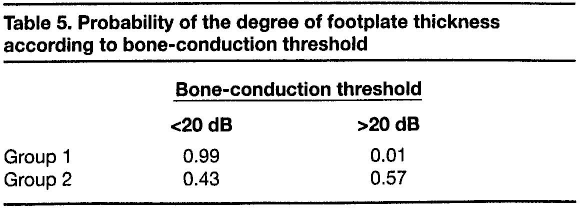
The mean preoperative Carhart notches in group 1 and group 2 were 9.6 ± 7.9 dB and 10 ± 12.7 dB, respectively—not a significant difference (p = 0.9). Most patients in group 1 had a bone-conduction threshold less than 20 dB, while most of those in group 2 had a higher bone-conduction threshold. Table 5 shows the probability of footplate thickness corresponding to bone-conduction threshold in the two groups.
Probability of the degree of footplate thickness according to bone-conduction threshold
Air-bone gaps
The mean preoperative air-bone gaps were 31.7 ± 9.2 dB in group land 34.3 ± 13.1 dB in group 2. The difference was not statistically significant (p=0.4).
Discussion
Overall, the incidence of otosclerosis is much lower in men than in women.3,12 The female-to-male ratio in our study was 1.1:1. We found no significant relationship between sex and footplate thickness, or between age and thickness.
On histologic analysis of stapes footplate fragments, the pathologic process in otosclerosis can be classified into three stages: spongiotic, fibrotic, and sclerotic. There is a direct correlation between the stage of otosclerosis and the age of patients. 2
In our study, we classified footplate thickness into four grades and then, for more reliability, into two groups. It appears that there was a direct relationship between higher bone-conduction thresholds and greater footplate thickness. We also expected to find a relationship between air-bone gaps and footplate thickness, but our findings in this regard were not statistically significant. Instead, we noticed that when bone-conduction thresholds were less than 20 dB, the likelihood of having a thick footplate decreased. Also, we did not find any association between the thickness of the footplate and the histologic stage of the otosclerotic lesion.
In a study by Gros et al, histologic examination of the stapes footplate fragments revealed that most otosclerotic lesions were fibrotic; among the remainder, sclerotic lesions were more common than spongiotic lesions. 2 This is probably an indication that otosclerosis is a dynamic disease, and after the early spongiotic type progresses toward the fibrotic phase, the disease then enters what is variously called a mature, inactive, or sclerotic phase.
Although Gros et al found no significant associations among (1) the phase of the otosclerotic lesion, (2) the level of preoperative conductive hearing loss, and (3) the degree of sensorineural hearing loss, they did find that mean preoperative air- and bone-conduction thresholds and air-bone gaps were worse in patients with the fibrotic type of otosclerotic lesion than the spongiotic type, and that they were the worst in those with the sclerotic type. 2 Recently, histologic studies have demonstrated that the production of tumor necrosis factor alpha in active otosclerosis might be responsible for sensorineural hearing loss in this disease. 13
Cherukupally et al showed that bony ankylosis of the footplate was associated with an air-bone gap of greater than 30 dB. 14 However, they reported that the air-bone gap could not reliably predict the degree and extent of bony footplate ankylosis.
Our study protocol would have been better if we had been able to use a measurement technique to assess footplate thickness more precisely and if we could have eliminated all bias. Because three different surgeons were involved, we were concerned about interobserver bias, as mentioned previously. We tried to minimize it by consolidating our data from four small sets and placing it into two larger groups with a more discrete definition of the criteria.
Stapes surgery requires complex surgical skills and experience to achieve good results. 15 In order to make an estimation of the thickness of the footplate and the amount of drilling required to create a fenestra, several studies have tried to establish the value of multislice computed tomography (CT) in otosclerosis. 16 It seems that using audiometry as an indicator is easier and more acceptable than using CT to predict such data. However, Genç and Sennaroğlu showed that there was no difference between bone-conduction thresholds in obliterative otosclerosis and those of the annular form. 17
Our study showed that when operating on otosclerotic patients who have high hearing thresholds, surgeons may encounter higher grades of footplate thickness intraoperatively. Greater footplate thickness in stapedectomy requires greater surgical skills. Therefore, measuring the thickness of the footplate prior to surgery may help us to be more vigilant and prepared for the difficulties that we might face during the operation.
Malafronte et al have proposed a new classification system for otosclerosis: blue otosclerosis (blue footplate), white otosclerosis (white footplate), and obliterative oto-sclerosis (footplate not visible). 18 They recommend using this classification before performing any manipulation of the stapes, in order to identify the different degrees of difficulty of surgery. However, the ability to predict the difficulty of surgery before going to the operating room with an objective measurement like pure-tone audiometry would be more helpful in teaching hospital settings, where residents are being trained for these operations and are allowed to operate on some patients.
More studies that measure footplate thickness as a quantitative parameter and the relationship between footplate thickness and the histologic pattern of oto-sclerotic lesions are needed.