
Abstract
We conducted a study to examine cochlear activity in women with a naturally occurring menstrual cycle by measuring transient otoacoustic emissions (TOAEs) and distortion-product otoacoustic emissions (DPOAEs). Our study population was made up of 11 women aged 20 to 40 years (mean: 35.6) who were not taking a contraceptive medication or hormone therapy. Measurements of TOAEs and DPOAEs were made during both the follicular phase and the luteal phase of the menstrual cycle. We found no statistically significant difference in any of the TOAE amplitude values between the two phases. Although a sharp decrease at the 0.75 kHz frequency was seen in DPOAEs during both phases, none of the amplitude values in the tested frequencies were significantly different between the two phases. The absence of TOAE and DPOAE amplitude changes suggests that it is unnecessary to take into account the phase of the menstrual cycle when interpreting the results of otoacoustic emissions testing.
Introduction
The menstrual cycle is divided into three phases: follicular, ovulatory, and luteal. The follicular phase starts with menstrual bleeding and lasts about 15 days. After ovulation, the luteal phase begins; it lasts about 13 to 15 days and ends with the next onset of menses. In the luteal phase, progesterone levels increase and levels of luteinizing hormone/follicle-stimulating hormone (LH/ FSH) and estrogen decrease. High progesterone levels may increase sodium, chloride, and water reabsorption. The menstrual cycle ends when progesterone and LH/FSH levels are at a minimum.
Homeostasis and the biochemical status of inner ear fluids are essential for balance and for hearing. Women with naturally occurring menstrual cycles may experience fluctuations in auditory and labyrinthine functions during certain times in their menstrual cycle. 1 The physiologic basis of this relationship is unclear. Menstrual cycle variations in sodium and water absorption/reabsorption and hormonal influences on cochlear blood flow affect the active mechanism of the cochlea.2,3
It has been proposed that the frequencies of otoacoustic emissions (OAEs) may be used to assess such variations during the different phases of the cycle. Therefore, we conducted a study to examine the hair cell activity in women during a normal menstrual cycle. Our goal was to ascertain the effects of hormone variations in cycle phases by means of measuring transient otoacoustic emissions (TOAEs) and distortion-product otoacoustic emissions (DPOAEs).
Subjects and methods
Our study population was made up of 11 women aged 20 to 40 years (mean: 35.6) who were not taking any contraceptive agents or hormone therapy. All were interviewed to obtain an otologic history and information about their use of medications and their menstrual cycles. The history and findings on routine ENT examination (otoscopy) and pure-tone audiometry were within normal limits, and there were no impediments to OAE testing.
Once the absence of auditory pathology was confirmed, the assessment of TOAEs and DPOAEs was made. These tests were conducted in a sound-proofroom. Each woman underwent two testing sessions: once during the follicular phase and once during the luteal phase. TOAE testing involved an acoustic stimulus of very short duration (clicks), and DPOAE testing involved two simultaneous tones of different frequencies (f1–f2). TOAEs were considered present when 1.0 and 1.5 kHz frequency amplitudes were 3 dB or higher and when 2.0, 3.0, and 4.0 kHz frequency amplitudes were 6 dB or higher. DPOAEs were considered present when the difference between amplitude and noise was greater than 6 dB.
Multivariate data analysis was performed with the Statistical Package for the Social Sciences software (v. 13.0; SPSS; Chicago) to assess the effect of the phase of the menstrual cycle on OAEs.
The study protocol was approved by the Research Ethics Committee of the Gaziosmanpasa University Faculty of Medicine, and written informed consent was obtained from all patients.
Results
There was no statistically significant difference in mean TOAE amplitudes at 1.0, 1.5, 2.0, 3.0, and 4.0 kHz between the follicular phase (figure 1) and the luteal phase (figure 2).
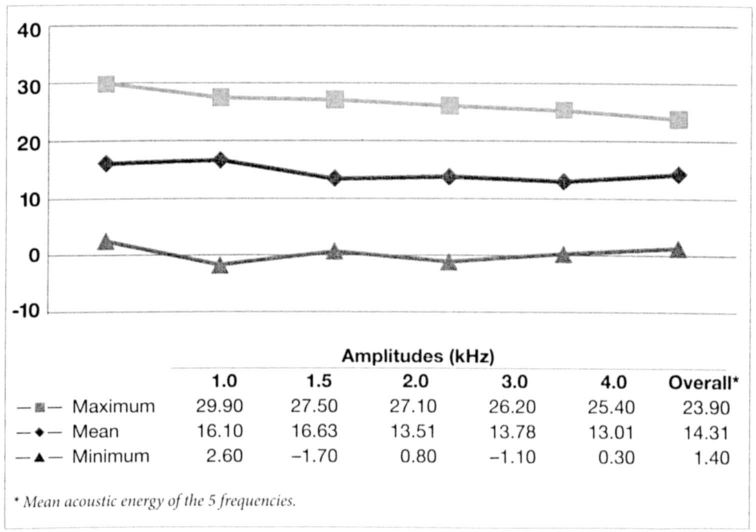
TOAE amplitudes during the follicular phase.
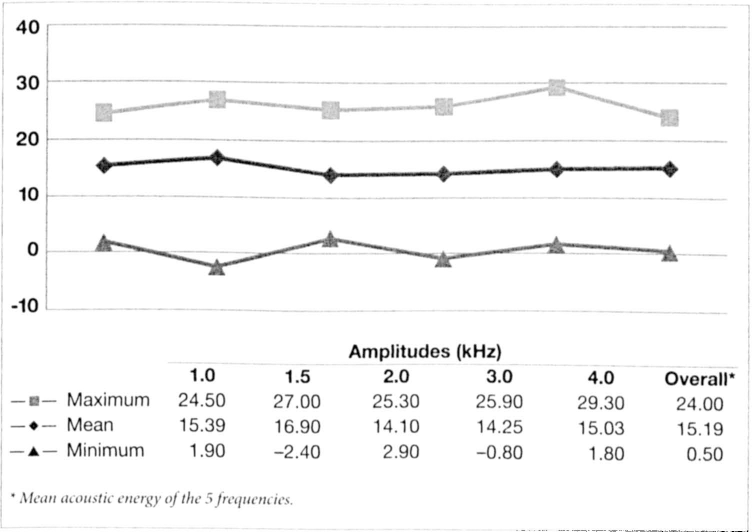
TOAE amplitudes during the luteal phase.
Likewise, there was no significant difference in mean DPOAE amplitudes at 0.75, 1.0, 1.5, 2.0, 3.0, 4.0, 6.0, and 8.0 kHz between the follicular phase (figure 3) and the luteal phase (figure 4). Of note, a sharp decrease was seen at 0.75 kHz during both phases.
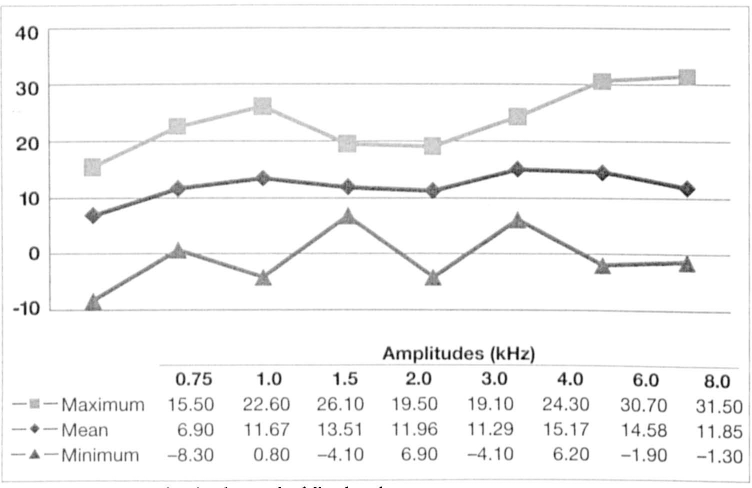
DPOAE amplitudes during the follicular phase.
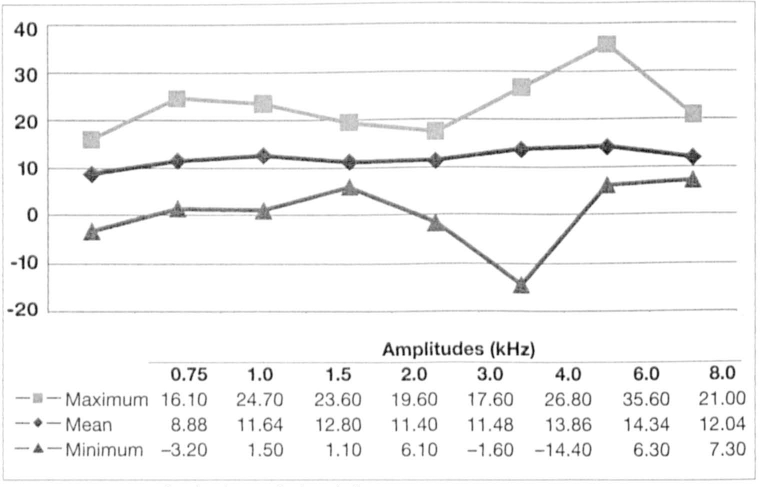
DPOAE amplitudes during the luteal phase.
Discussion
OAEs are the sounds generated by contractions of the outer hair cells following the presentation of a sound stimulus. They can occur spontaneously, and they can be evoked. Evoked OAEs are produced by either a click (evoked TOAEs) or two pure sounds (evoked DPOAEs), and they represent a release of acoustic energy picked up in the external auditory canal in response to the acoustic stimuli. TOAEs and DPOAEs are reflections of the same cochlear phenomenon, and the presence of either type of emission suggests normal cochlear function. The presence of OAEs is correlated with normal outer hair cell function.
TOAE and DPOAE tests are essentially screening tools; they cannot be used to predict or determine the degree of hearing loss because neither can be reliably recorded in ears that have conductive pathology or in patients who have more than a moderate degree of sensorineural hearing loss. Still, OAE testing has proved to be a valuable initial tool for evaluating auditory function in children and adults.
It has been proposed that changes in hearing function among women may occur as a result of menses-associated variations in cochlear blood flow and/or changes in those outer hair cells that are sensitive to metabolic and hormonal fluctuations. 4 However, only a limited number of studies of OAEs in women have been published.
Fluctuations in the frequencies of spontaneous OAEs have been reported.5,6 These frequencies were found to decline before the onset of menstruation and to rise to a peak near the suspected time of ovulation. Penner examined the frequencies of 1 woman's spontaneous OAEs intermittently for 295 days and found that anovulation, as evidenced by amenorrhea or induced by oral contraception, reduced the fluctuation of spontaneous OAE frequencies relative to the naturally occurring menstrual cycle. 5 Bell found that the frequencies of spontaneous OAEs directly corresponded to fluctuations in estradiol concentrations during the cycle. 6
On the other hand, Yellin and Stillman studied the influences of the menstrual cycle on the amplitude values of evoked TOAEs and DPOAEs in 13 normal-hearing, normal-cycling women. 7 They found no systematic amplitude changes and no correlation with phases of the menstrual cycle, and they concluded that evoked OAEs are unaffected by physiologic changes associated with the menstrual cycle.
Likewise, Arruda and Silva assessed 21 women aged 20 to 35 years who did not take any contraceptive medicine by TOAE and DPOAE testing during the three phases of the menstrual cycle. 8 While the authors noticed a difference between right and left ears (DPOAEs at 1.5 kHz were higher on the right side), they found no statistically significant differences in TOAEs and DPOAEs during any of the phases.
An important factor that limits the usefulness of spontaneous OAEs is that they occur in only 40 to 50% of normal-hearing individuals.4–6 So while the presence of spontaneous OAEs is usually considered a sign of good cochlear health, their absence is not necessarily a sign of audiologic pathology. Therefore, we did not evaluate spontaneous OAEs in our subjects.
None of our subjects used anovulatory contraceptives during the study, nor did they experience other hormonal changes such as amenorrhea or menopause. We excluded such women because these factors can affect the dynamics of OAE frequencies. Our finding that there was no significant correlation between TOAEs and DPOAEs and the phases of the menstrual cycle suggest that it is unnecessary to take the phase of the menstrual cycle into account when interpreting OAE test results.