
Abstract

A 68-year-old man, a retired counselor, had a “raspy” voice throughout his entire life. He reported hoarseness, difficulty speaking loudly, and vocal fatigue. His vocal handicap index (VHI) was 53.
Strobovideolaryngoscopy revealed bilateral sulcus vocalis (figure 1). This congenital lesion results in deficiency or absence of the superficial layer of the lamina propria. Figure 2 shows an ellipsoidal area along the left vocal fold where there is only a thin layer of epithelium over the vocal ligament.
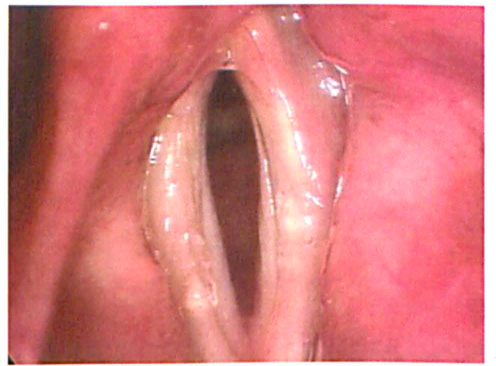
Strobovideolaryngoscopy reveals bilateral sulcus vocalis.
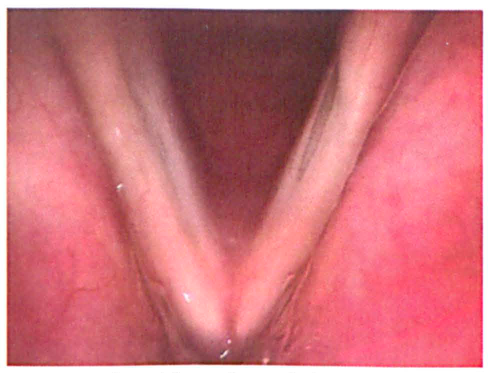
An ellipsoidal area of particularly severe involvement is seen along the left vocal fold, in which thin epithelium is adherent to the vocal ligament.
In sulcus vocalis, either the superficial layer of the lamina propria is absent altogether (usually causing severe dysphonia and requiring considerable vocal effort), or a portion of the epithelium invaginates through the superficial layer of the lamina propria and adheres to the vocal ligament. Typically, there is an increase in collagen fibers and deficiency of capillaries in the region of the sulcus. Sulcus results in stiffness of the vibratory margin of the vocal folds, and often in adynamic segments. This produces hoarseness, breathiness, increased phonation threshold pressures, decreased vocal efficiency and, commonly, voice fatigue.
Sulcus vocalis must be differentiated from sulcus vergeture, which may present a similar appearance. However, sulcus vergeture is caused by atrophic changes in the epithelium and sometimes thinning of the superficial layer of the lamina propria; but the epithelium is not attached to the vocal ligament, and symptoms generally are not as severe as they are in sulcus vocalis. In fact, sulcus vergeture may be asymptomatic.